

Can an Arthroplasty Registry Help Decrease Transfusions in Primary Total Joint Replacement? A Quality Initiative
- PMID: 26215083
- PMCID: PMC4686507
- DOI: 10.1007/s11999-015-4470-z
Can an Arthroplasty Registry Help Decrease Transfusions in Primary Total Joint Replacement? A Quality Initiative
Erratum in
-
Erratum to: Can an Arthroplasty Registry Help Decrease Transfusions in Primary Total Joint Replacement? A Quality Initiative.Clin Orthop Relat Res. 2016 Jan;474(1):279. doi: 10.1007/s11999-015-4557-6. Clin Orthop Relat Res. 2016. PMID: 26452747 Free PMC article. No abstract available.
Abstract
Background: Standardized care plans are effective at controlling cost and quality. Registries provide insights into quality and outcomes for use of implants, but most registries do not combine implant and care quality data. In 2012, several Michigan area hospitals and a major insurance provider formed a voluntary statewide total joint database/registry, the Michigan Arthroplasty Registry Collaborative Quality Initiative (MARCQI), to collect procedural, hospital, discharge, and readmission data. Noting substantial variation in transfusion practices after total joint arthroplasty (TJA) in our institutions, we used these prospectively collected data to examine whether awareness and education of the American Association of Blood Banks' (AABB) transfusion guidelines would result in decreased transfusions.
Questions/purposes: (1) Can an established arthroplasty registry help implement a quality initiative (QI) designed to decrease the proportion of transfused postoperative patients undergoing TJA? (2) Do data-driven transfusion protocols decrease length of stay without increasing ischemic complications (myocardial infarctions and cerebrovascular accidents)? (3) Are decreased transfusion proportions associated with decreased readmissions, nonischemic morbidity (including deep vein thrombosis and deep prosthetic infection), and mortality in postoperative patients who had undergone TJA?
Methods: After reviewing data from the recently established MARCQI registry, the orthopaedic department noticed many discrepancies and practice variances regarding blood transfusions among their providers. In October 2013, a QI was implemented to raise awareness of the discrepancies and education about the AABB guidelines was presented at the monthly orthopaedic service line meeting. A total of 1872 TJA cases were reviewed; 50 were excluded for incomplete data and two for intraoperative transfusions for the period before education (May 2012 to June 2013, n = 1240) and after education (November 2013 to April 2014, n = 580). Data collected included gender, age, length of stay, body mass index, preoperative hemoglobin level, lowest postoperative hemoglobin level during admission, transfusion status, number of units transfused, ischemic and nonischemic morbidity, hospital readmissions within 90 days, and mortality. Pre- and post-QI transfusion proportions were calculated. Chi-square test, Student's t-test, and a multivariate analysis were performed to compare differences in transfusion proportions for patients with a postoperative hemoglobin ≥ 8 g/dL.
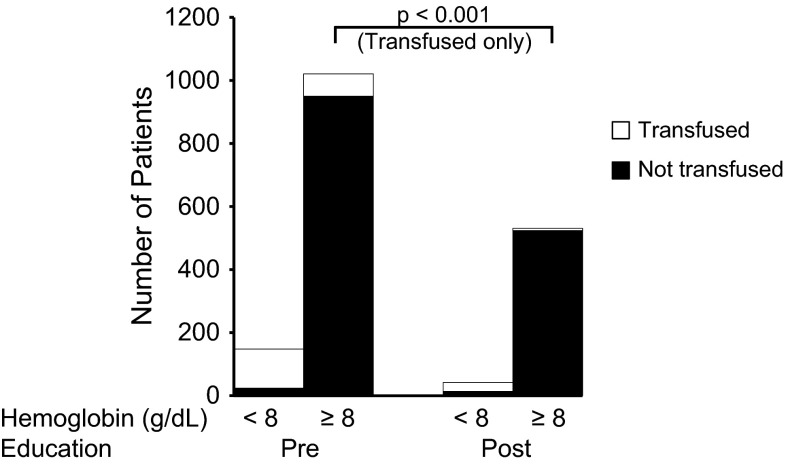
Results: Overall, the percentage of patients transfused with a postoperative hemoglobin ≥ 8 g/dL decreased 80% (6.5% [71 of 1092] versus 1.3% [seven of 538]; odds ratio, 5.3; 95% confidence interval, 2.4-11.6; p < 0.001) after the educational intervention. Before education, 16% (195 of 1240) of all patients undergoing TJA were transfused, whereas 6.5% (71 of 1092) were outside recommended AABB guidelines (hemoglobin ≥ 8 g/dL). In the 6 months after QI initiation, overall transfusions decreased to 6% (35 of 580) with 1.3% (seven of 538) having a hemoglobin ≥ 8 g/dL. The mean length of stay for nontransfused patients was shorter (2.4 days ± 0.9 versus 3.3 days ± 1.1, p < 0.001) and ischemic complications did not differ between groups (0.32% [four of 1240] versus 0.34% [two of 580], p = 0.61). Before and after education, neither the number of readmissions (5.4% [67 of 1240] versus 4.7% [27 of 580], p = 0.50) nor morbidity (3.6% [45 of 1240] versus 2.4% [14 of 580], p = 0.17) differed between time periods. There were no deaths.
Conclusions: Simple education and awareness of quality practices drive safety and compliance. The impact can be immediate and lasting. Arthroplasty registries that combine procedural and care quality data are vital and may be used for important data-driven QIs.
Level of evidence: Level III, therapeutic study.
Figures
Comment in
-
CORR Insights(®): Can an Arthroplasty Registry Help Decrease Transfusions in Primary Total Joint Replacement? A Quality Initiative.Clin Orthop Relat Res. 2016 Jan;474(1):132-3. doi: 10.1007/s11999-015-4508-2. Epub 2015 Aug 18. Clin Orthop Relat Res. 2016. PMID: 26280683 Free PMC article. No abstract available.
References
-
- Bierbaum B, Callaghan J, Galante J, Rubash H, Tooms R, Welch R. An analysis of blood management in patients having a total hip or knee arthroplasty. J Bone Joint Surg Am. 1999;81:2–10. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
