

Incidence of gastric cancer among patients with gastric precancerous lesions: observational cohort study in a low risk Western population
- PMID: 26215280
- PMCID: PMC4516137
- DOI: 10.1136/bmj.h3867
Incidence of gastric cancer among patients with gastric precancerous lesions: observational cohort study in a low risk Western population
Erratum in
-
Incidence of gastric cancer among patients with gastric precancerous lesions: observational cohort study in a low risk Western population.BMJ. 2015 Jul 29;351:h4134. doi: 10.1136/bmj.h4134. BMJ. 2015. PMID: 26223234 Free PMC article. No abstract available.
Abstract
Objective: To accurately measure the incidence of gastric cancer among patients with gastric precancerous lesions, and to quantify the excess incidence in comparison with people with normal mucosa on endoscopy and a general population.
Design: Population based cohort study.
Setting: Population of Sweden using data from its national disease registers.
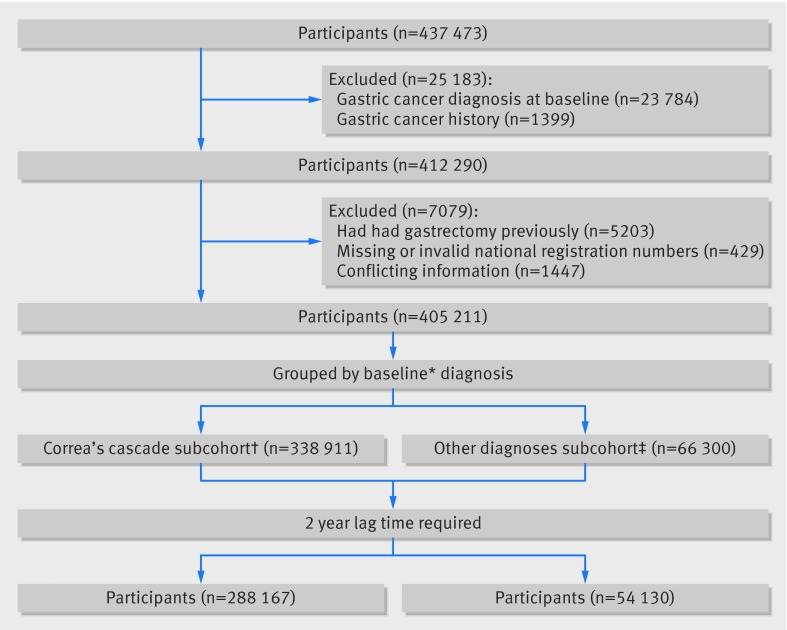
Participants: 405,172 patients who had gastric biopsy samples taken for non-malignant indications between 1979 and 2011.
Main outcome measures: Incidence of gastric cancer, reported separately for patients with different mucosal changes in biopsy samples. Standardised incidence ratios provided estimation of the relative risk, using the general Swedish population as reference; and hazard ratios were derived from Cox regression modelling for internal comparisons with patients with normal gastric mucosa.
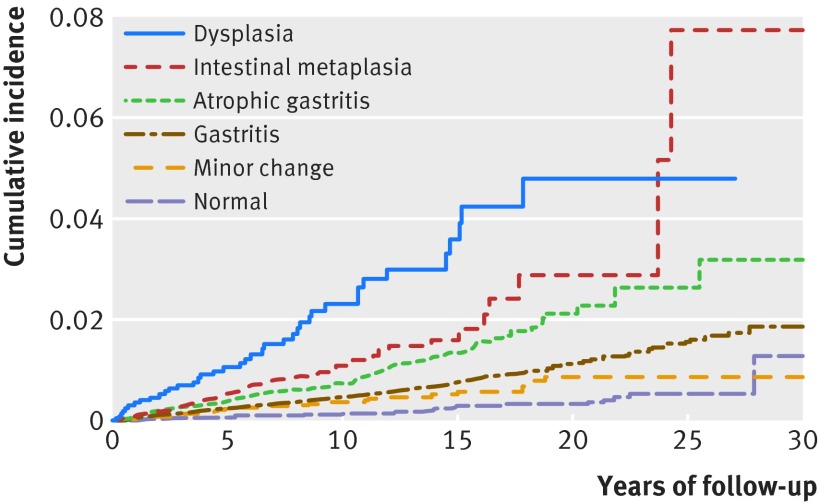
Results: After excluding the first two years of follow-up, 1599 cases of gastric cancer were identified. The annual crude incidence of gastric cancer was 20 × 10(-5) for those in the normal mucosa group (standardised incidence ratio 1.0), 42 × 10(-5) for those with minor changes (1.5), 59 × 10(-5) for the gastritis group (1.8), 100 × 10(-5) for the atrophic gastritis group (2.8), 129 × 10(-5) for the intestinal metaplasia group (3.4), and 263 × 10(-5) for the dysplasia group (6.5). Cox regression modelling confirmed that excess risks increased monotonically with progressive severity of gastric lesions, with the highest hazard ratio of 10.9 (dysplasia versus normal mucosa, 95% confidence interval 7.7 to 15.4). The increased incidence was stable throughout the follow-up period, and the gaps between cumulative incidence curves grew continuously.
Conclusions: Among patients who undergo gastroscopy with biopsy for clinical indications, approximately 1 in 256 with normal mucosa, 1 in 85 with gastritis, 1 in 50 with atrophic gastritis, 1 in 39 with intestinal metaplasia, and 1 in 19 with dysplasia will develop gastric cancer within 20 years. These numbers, along with cost-benefit analyses, should guide future surveillance policies for these particular patient groups.
© Song et al 2015.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures

References
-
- Kapadia CR. Gastric atrophy, metaplasia, and dysplasia: a clinical perspective. J Clin Gastroenterol 2003;36(5 Suppl):S29-36, S61-2. - PubMed
-
- Correa P. Human gastric carcinogenesis: a multistep and multifactorial process—first American Cancer Society award lecture on cancer epidemiology and prevention. Cancer Res 1992;52:6735-40. - PubMed
-
- Lauren P. The two histological main types of gastric carcinoma: diffuse and so-called intestinal-type carcinoma. An attempt at a histo-clinical classification. Acta Pathol Microbiol Scand 1965;64:31-49. - PubMed
-
- IARC working group on the evaluation of carcinogenic risks to humans: some industrial chemicals. Lyon, 15-22 February 1994. IARC Monogr Eval Carcinog Risks Hum 1994;60:1-560.
-
- Konturek PC, Konturek SJ, Brzozowski T. Helicobacter pylori infection in gastric cancerogenesis. J Physiol Pharmacol 2009;60:3-21. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical