

Visit-to-Visit Variability of Blood Pressure and Coronary Heart Disease, Stroke, Heart Failure, and Mortality: A Cohort Study
- PMID: 26215765
- PMCID: PMC5021508
- DOI: 10.7326/M14-2803
Visit-to-Visit Variability of Blood Pressure and Coronary Heart Disease, Stroke, Heart Failure, and Mortality: A Cohort Study
Abstract
Background: Variability of blood pressure (BP) across outpatient visits is frequently dismissed as random fluctuation around a patient's underlying BP.
Objective: To examine the association of visit-to-visit variability (VVV) of systolic BP (SBP) and diastolic BP with cardiovascular disease (CVD) and mortality outcomes.
Design: Prospective cohort study.
Setting: Post hoc analysis of ALLHAT (Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial).
Participants: 25 814 ALLHAT participants.
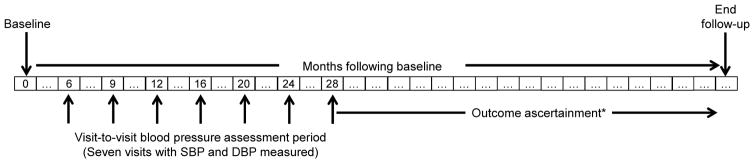
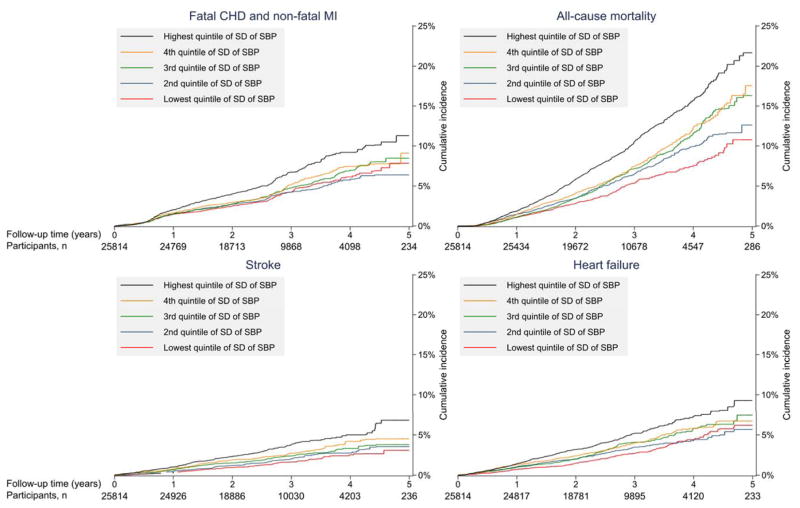
Measurements: The VVV of SBP was defined as the SD across SBP measurements obtained at 7 visits conducted from 6 to 28 months after ALLHAT enrollment. Participants without CVD events during the first 28 months of follow-up were followed from the 28-month visit through the end of active ALLHAT follow-up. Outcomes included fatal coronary heart disease (CHD) or nonfatal myocardial infarction, all-cause mortality, stroke, and heart failure.
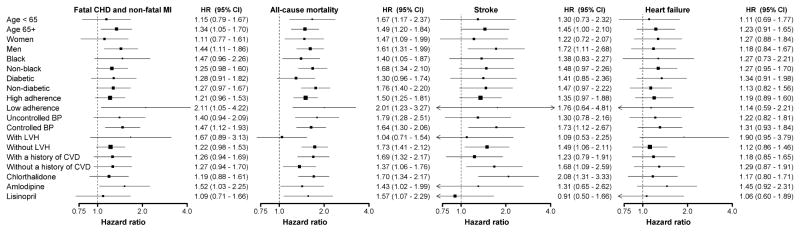
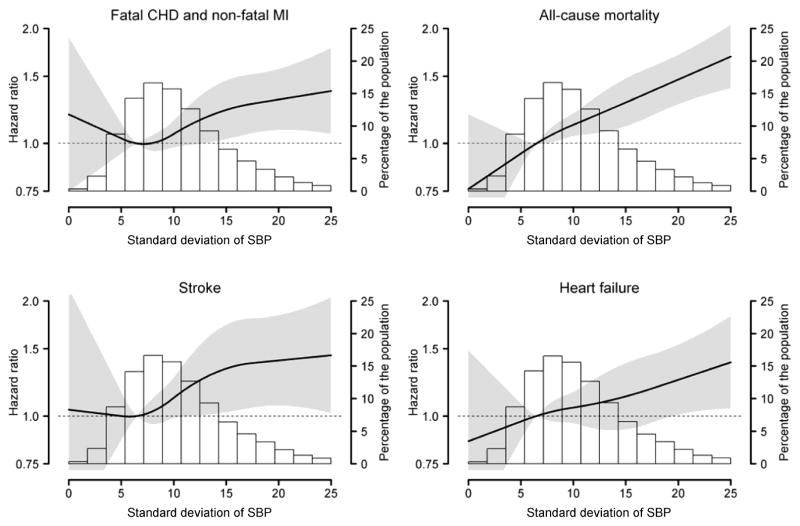
Results: During follow-up, 1194 fatal CHD or nonfatal MI events, 1948 deaths, 606 strokes, and 921 heart failure events occurred. After multivariable adjustment, including for mean SBP, the hazard ratio comparing participants in the highest versus lowest quintile of SD of SBP (≥14.4 mm Hg vs. <6.5 mm Hg) was 1.30 (95% CI, 1.06 to 1.59) for fatal CHD or nonfatal MI, 1.58 (CI, 1.32 to 1.90) for all-cause mortality, 1.46 (CI, 1.06 to 2.01) for stroke, and 1.25 (CI, 0.97 to 1.61) for heart failure. Higher VVV of diastolic BP was also associated with CVD events and mortality.
Limitation: Long-term outcomes were not available.
Conclusion: Higher VVV of SBP is associated with an increased risk for CVD and mortality. Future studies should examine whether reducing VVV of BP lowers this risk.
Primary funding source: National Institutes of Health.
Figures
Comment in
-
Blood pressure variability is associated with increased risk of heart disease and death, study finds.BMJ. 2015 Jul 27;351:h4080. doi: 10.1136/bmj.h4080. BMJ. 2015. PMID: 26219653 No abstract available.
-
Celebrating the ACP Centennial: From the Annals Archive-Blood Pressure Variation.Ann Intern Med. 2015 Sep 1;163(5):389. doi: 10.7326/M15-1637. Ann Intern Med. 2015. PMID: 26322698 No abstract available.
-
Variability May Be the "Law of Life," but Blood Pressure Variability May Forebode a Shorter Life.Am J Kidney Dis. 2016 Jun;67(6):830-3. doi: 10.1053/j.ajkd.2016.01.014. Epub 2016 Feb 18. Am J Kidney Dis. 2016. PMID: 26898700 Free PMC article. No abstract available.
Summary for patients in
-
Summaries for Patients. Variation in Blood Pressure Readings and the Risk for Cardiovascular Disease.Ann Intern Med. 2015 Sep 1;163(5). doi: 10.7326/P15-9027. Ann Intern Med. 2015. PMID: 26215385 No abstract available.
References
-
- Pickering TG, Hall JE, Appel LJ, et al. Recommendations for blood pressure measurement in humans and experimental animals: Part 1: blood pressure measurement in humans: a statement for professionals from the Subcommittee of Professional and Public Education of the American Heart Association Council on High Blood Pressure Research. Hypertension. 2005;45(1):142–161. - PubMed
-
- Clarke R, Shipley M, Lewington S, et al. Underestimation of risk associations due to regression dilution in long-term follow-up of prospective studies. Am J Epidemiol. 1999 Aug 15;150(4):341–353. - PubMed
-
- MacMahon S, Peto R, Cutler J, et al. Blood pressure, stroke, and coronary heart disease: Part 1, prolonged differences in blood pressure: prospective observational studies corrected for the regression dilution bias. Lancet. 1990 Mar 31;335:765–774. - PubMed
-
- Rothwell PM, Howard SC, Dolan E, et al. Prognostic significance of visit-to-visit variability, maximum systolic blood pressure, and episodic hypertension. Lancet. 2010 Mar 13;375(9718):895–905. - PubMed
-
- Muntner P, Shimbo D, Tonelli M, Reynolds K, Arnett DK, Oparil S. The relationship between visit-to-visit variability in systolic blood pressure and all-cause mortality in the general population: findings from NHANES III, 1988 to 1994. Hypertension. 2011 Feb;57(2):160–166. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical