

Systolic left ventricular function is preserved during therapeutic hypothermia, also during increases in heart rate with impaired diastolic filling
- PMID: 26215808
- PMCID: PMC4513019
- DOI: 10.1186/s40635-015-0041-6
Systolic left ventricular function is preserved during therapeutic hypothermia, also during increases in heart rate with impaired diastolic filling
Abstract
Background: Systolic left ventricular function during therapeutic hypothermia is found both to improve and to decline. We hypothesized that this discrepancy would depend on the heart rate and the variables used to assess systolic function.
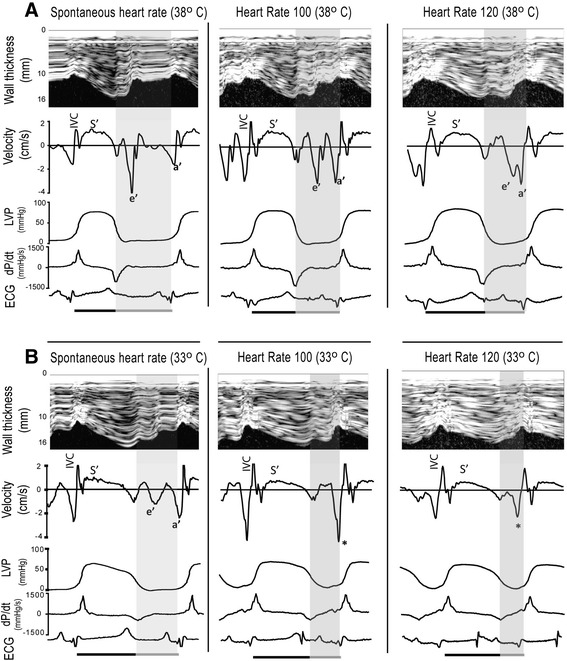
Methods: In 16 pigs, cardiac performance was assessed by measurements of invasive pressures and thermodilution cardiac output and with 2D strain echocardiography. Left ventricle (LV) volumes, ejection fraction (EF), transmitral flow, and circumferential and longitudinal systolic strain were measured. Miniaturized ultrasonic transducers were attached to the epicardium of the LV to obtain M-mode images, systolic thickening, and diastolic thinning velocities and to determine LV pressure-wall dimension relationships. Preload recruitable stroke work (PRSW) was calculated. Measurements were performed at 38 and 33°C at spontaneous and paced heart rates, successively increased in steps of 20 up to the toleration limit. Effects of temperature and heart rate were compared in a mixed model analysis.
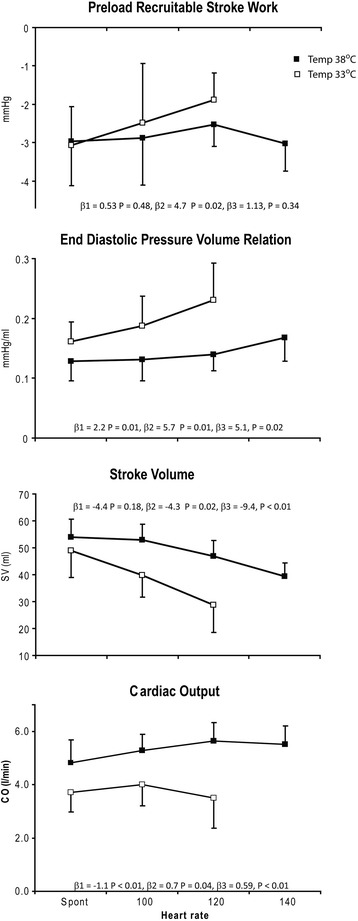
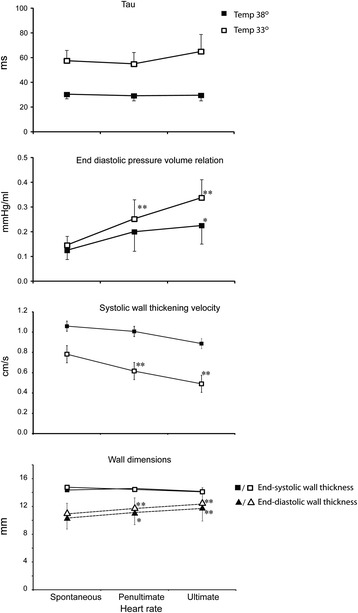
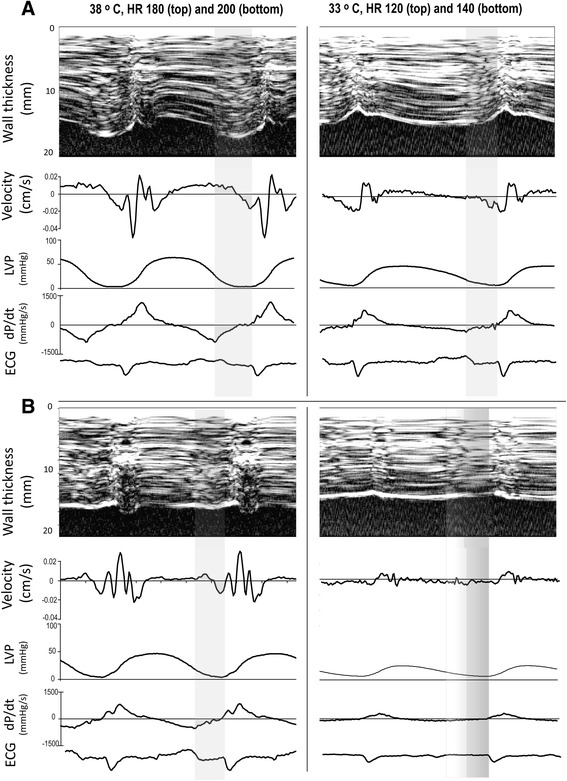
Results: Hypothermia reduced heart rate from 87 ± 10 (SD) to 76 ± 11 beats/min without any changes in LV stroke volume, end-diastolic volume, EF, strain values, or PRSW. Systolic wall thickening velocity (S') and early diastolic wall thinning velocity decreased by approximately 30%, making systolic duration longer through a prolonged and slow contraction and changing the diastolic filling pattern from predominantly early towards late. Pacing reduced diastolic duration much more during hypo- than during normothermia, and combined with slow myocardial relaxation, incomplete relaxation occurred with all pacing rates. Pacing did not affect S' or PRSW at physiological heart rates, but stroke volume, end-diastolic volume, and strain were reduced as a consequence of reduced diastolic filling and much more accentuated during hypothermia. At the ultimate tolerable heart rate during hypothermia, S' decreased, probably as a consequence of myocardial hypoperfusion due to sustained ventricular contraction throughout a very short diastole.
Conclusions: Systolic function was maintained at physiological heart rates during therapeutic hypothermia. Reduced tolerance to increases in heart rate was caused by lack of ventricular filling due to diastolic dysfunction and shorter diastolic duration.
Figures
References
-
- Nielsen N, Wetterslev J, Cronberg T, Erlinge D, Gasche Y, Hassager C, Horn J, Hovdenes J, Kjaergaard J, Kuiper M, Pellis T, Stammet P, Wanscher M, Wise MP, Aneman A, Al-Subaie N, Boesgaard S, Bro-Jeppesen J, Brunetti I, Bugge JF, Hingston CD, Juffermans NP, Koopmans M, Kober L, Langorgen J, Lilja G, Moller JE, Rundgren M, Rylander C, Smid O, Werer C, Winkel P, Friberg H. Targeted temperature management at 33 degrees C versus 36 degrees C after cardiac arrest. N Engl J Med. 2013;369:2197–2206. doi: 10.1056/NEJMoa1310519. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
