

Alveolar instability (atelectrauma) is not identified by arterial oxygenation predisposing the development of an occult ventilator-induced lung injury
- PMID: 26215818
- PMCID: PMC4480795
- DOI: 10.1186/s40635-015-0054-1
Alveolar instability (atelectrauma) is not identified by arterial oxygenation predisposing the development of an occult ventilator-induced lung injury
Abstract
Background: Improperly set mechanical ventilation (MV) with normal lungs can advance lung injury and increase the incidence of acute respiratory distress syndrome (ARDS). A key mechanism of ventilator-induced lung injury (VILI) is an alteration in alveolar mechanics including alveolar instability or recruitment/derecruitment (R/D). We hypothesize that R/D cannot be identified by PaO2 (masking occult VILI), and if protective ventilation is not applied, ARDS incidence will increase.
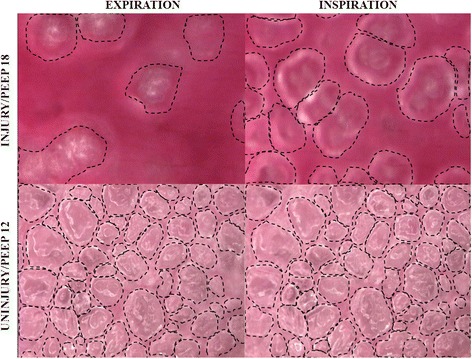
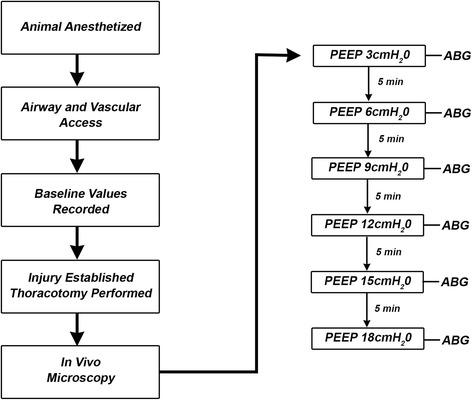
Methods: Sprague-Dawley rats (n = 8) were anesthetized, surgically instrumented, and placed on MV. A thoracotomy was performed and an in vivo microscope attached to the pleural surface of the lung with baseline dynamic changes in alveolar size during MV recorded. Alveolar instability was induced by intra-tracheal instillation of Tween and alveolar R/D identified as a marked change in alveolar size from inspiration to expiration with increases in positive end-expiratory pressure (PEEP) levels.
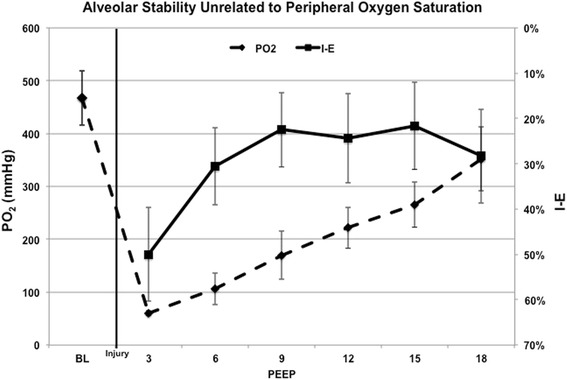
Results: Despite maintaining a clinically acceptable PaO2 (55-80 mmHg), the alveoli remained unstable with significant R/D at low PEEP levels. Although PaO2 consistently increased with an increase in PEEP, R/D did not plateau until PEEP was >9 cmH2O.
Conclusions: PaO2 remained clinically acceptable while alveolar instability persisted at all levels of PEEP (especially PEEP <9 cmH2O). Therefore, PaO2 levels cannot be used reliably to guide protective MV strategies or infer that VILI is not occurring. Using PaO2 to set a PEEP level necessary to stabilize the alveoli could underestimate the potential for VILI. These findings highlight the need for more accurate marker(s) of alveolar stability to guide protective MV necessary to prevent VILI.
Figures
Similar articles
-
Personalizing mechanical ventilation according to physiologic parameters to stabilize alveoli and minimize ventilator induced lung injury (VILI).Intensive Care Med Exp. 2017 Dec;5(1):8. doi: 10.1186/s40635-017-0121-x. Epub 2017 Feb 2. Intensive Care Med Exp. 2017. PMID: 28150228 Free PMC article. Review.
-
Injurious mechanical ventilation in the normal lung causes a progressive pathologic change in dynamic alveolar mechanics.Crit Care. 2007;11(3):R64. doi: 10.1186/cc5940. Crit Care. 2007. PMID: 17565688 Free PMC article.
-
Effect of positive end-expiratory pressure and tidal volume on lung injury induced by alveolar instability.Crit Care. 2007;11(1):R20. doi: 10.1186/cc5695. Crit Care. 2007. PMID: 17302983 Free PMC article.
-
Low-volume ventilation of preinjured lungs degrades lung function via stress concentration and progressive alveolar collapse.Am J Physiol Lung Cell Mol Physiol. 2024 Jul 1;327(1):L19-L39. doi: 10.1152/ajplung.00323.2023. Epub 2024 May 7. Am J Physiol Lung Cell Mol Physiol. 2024. PMID: 38712429
-
How respiratory system mechanics may help in minimising ventilator-induced lung injury in ARDS patients.Eur Respir J Suppl. 2003 Aug;42:15s-21s. doi: 10.1183/09031936.03.00420303. Eur Respir J Suppl. 2003. PMID: 12945996 Review.
Cited by
-
Prevention and treatment of acute lung injury with time-controlled adaptive ventilation: physiologically informed modification of airway pressure release ventilation.Ann Intensive Care. 2020 Jan 6;10(1):3. doi: 10.1186/s13613-019-0619-3. Ann Intensive Care. 2020. PMID: 31907704 Free PMC article. Review.
-
Alveolar dynamics during mechanical ventilation in the healthy and injured lung.Intensive Care Med Exp. 2019 Jul 25;7(Suppl 1):34. doi: 10.1186/s40635-019-0226-5. Intensive Care Med Exp. 2019. PMID: 31346797 Free PMC article. Review.
-
Ventilation and Perfusion at the Alveolar Level: Insights From Lung Intravital Microscopy.Front Physiol. 2020 Apr 3;11:291. doi: 10.3389/fphys.2020.00291. eCollection 2020. Front Physiol. 2020. PMID: 32308629 Free PMC article. Review.
-
Personalizing mechanical ventilation according to physiologic parameters to stabilize alveoli and minimize ventilator induced lung injury (VILI).Intensive Care Med Exp. 2017 Dec;5(1):8. doi: 10.1186/s40635-017-0121-x. Epub 2017 Feb 2. Intensive Care Med Exp. 2017. PMID: 28150228 Free PMC article. Review.
-
The Basic Science and Molecular Mechanisms of Lung Injury and Acute Respiratory Distress Syndrome.Int Anesthesiol Clin. 2018 Winter;56(1):1-25. doi: 10.1097/AIA.0000000000000177. Int Anesthesiol Clin. 2018. PMID: 29227309 Free PMC article. Review. No abstract available.
References
-
- Gajic O, Dara SI, Mendez JL, Adesanya AO, Festic E, Caples SM, Rana R, St Sauver JL, Lymp JF, Afessa B, Hubmayr RD. Ventilator-associated lung injury in patients without acute lung injury at the onset of mechanical ventilation. Crit Care Med. 2004;32:1817–1824. doi: 10.1097/01.CCM.0000133019.52531.30. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
