

Glucocorticoid-Induced Osteoporosis
- PMID: 26215995
- PMCID: PMC5905346
- DOI: 10.1007/978-1-4939-2895-8_8
Glucocorticoid-Induced Osteoporosis
Abstract
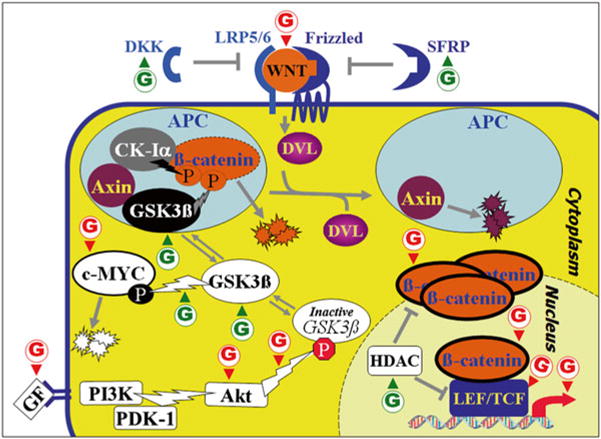
Osteoporosis is among the most devastating side effects of glucocorticoid (GC) therapy for the management of inflammatory and auto-immune diseases. Evidence from both humans and mice indicate deleterious skeletal effects within weeks of pharmacological GC administration, both related and unrelated to a decrease in bone mineral density (BMD). Osteoclast numbers and bone resorption are also rapidly increased, and together with osteoblast inactivation and decreased bone formation, these changes lead the fastest loss in BMD during the initial disease phase. Bone resorption then decreases to sub-physiological levels, but persistent and severe inhibition of bone formation leads to further bone loss and progressively increased fracture risk, up to an order of magnitude higher than that observed in untreated individuals. Bone forming osteoblasts are thus considered the main culprits in GC-induced osteoporosis (GIO). Accordingly, we focus this review primarily on deleterious effects on osteoblasts: inhibition of cell replication and function and acceleration of apoptosis. Mediating these adverse effects, GCs target pivotal regulatory mechanisms that govern osteoblast growth, differentiation and survival. Specifically, GCs inhibit growth factor pathways, including Insulin Growth Factors, Growth Hormone, Hepatocyte Growth/Scatter Factor and IL6-type cytokines. They also inhibit downstream kinases, including PI3-kinase and the MAP kinase ERK, the latter attributable in part to direct transcriptional stimulation of MAP kinase phosphatase 1. Most importantly, however, GCs inhibit the Wnt signaling pathway, which plays a pivotal role in osteoblast replication, function and survival. They transcriptionally stimulate expression of Wnt inhibitors of both the Dkk and Sfrp families, and they induce reactive oxygen species (ROS), which result in loss of ß-catenin to ROS-activated FoxO transcription factors. Identification of dissociated GCs, which would suppress the immune system without causing osteoporosis, is proving more challenging than initially thought, and GIO is currently managed by co-treatment with bisphosphonates or PTH. These drugs, however, are not ideally suited for GIO. Future therapeutic approaches may aim at GC targets such as those mentioned above, or newly identified targets including the Notch pathway, the AP-1/Il11 axis and the osteoblast master regulator RUNX2.
Figures
References
-
- Soen S, Tanaka Y. Glucocorticoid-induced osteoporosis: skeletal manifestations of glucocorticoid use and 2004 Japanese Society for Bone and Mineral Research-proposed guidelines for its management. Mod Rheumatol. 2005;15:163–8. - PubMed
-
- van Staa TP, et al. A simple score for estimating the long-term risk of fracture in patients using oral glucocorticoids. QJM. 2005;98:191–8. - PubMed
-
- Van Staa TP, Leufkens HG, Abenhaim L, Zhang B, Cooper C. Use of oral corticosteroids and risk of fractures. J Bone Miner Res. 2000;15:993–1000. - PubMed
-
- van Staa TP, Leufkens HG, Cooper C. The epidemiology of corticosteroid-induced osteoporosis: a meta-analysis. Osteoporos Int. 2002;13:777–87. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
