

Outbreak of Mycoplasma pneumoniae-Associated Stevens-Johnson Syndrome
- PMID: 26216320
- PMCID: PMC4516944
- DOI: 10.1542/peds.2015-0278
Outbreak of Mycoplasma pneumoniae-Associated Stevens-Johnson Syndrome
Erratum in
-
Olson et al. Outbreak of Mycoplasma pneumoniae-Associated Stevens Johnson Syndrome. Pediatrics. 2015;136(2):e386-394.Pediatrics. 2015 Dec;136(6):1198. doi: 10.1542/peds.2015-3276. Pediatrics. 2015. PMID: 26628717 Free PMC article. No abstract available.
Abstract
Background: Stevens-Johnson syndrome (SJS) is an uncommon, sporadic disease and outbreaks are rare. In November 2013, an outbreak of SJS was identified at Children's Hospital Colorado.
Methods: Outbreak cases were children aged 5-21 with a discharge diagnosis of SJS admitted from September 1 to November 30, 2013. Medical charts were reviewed using standardized data collection forms. Respiratory specimens were tested for viruses and Mycoplasma pneumoniae (Mp) by polymerase chain reaction (PCR). We conducted a separate 4-year retrospective case-control study comparing hospitalized SJS cases with and without evidence of Mp infection.
Results: During the outbreak, 8 children met SJS criteria. Median age was 11.5 years (range 8-16 years); 5 (63%) were boys and 5 (63%) were Mp-PCR-positive. Of the 5 PCR-positive children, none had preceding medication exposure, and all had radiographic pneumonia. All outbreak Mp isolates were macrolide susceptible. The retrospective case-control analysis showed that Mp-associated SJS episodes (n = 17) were more likely to have pneumonia (odds ratio [OR] 7.5, confidence interval [CI] 1.6–35.1), preceding respiratory symptoms (OR 30.0, CI 3.3–269.4) [corrected] an erythrocyte sedimentation rate ≥35 mg/dL (OR 22.8, CI 2.1-244.9), and ≤3 affected skin sites (OR 4.5, CI 1.2-17.4) than non-Mp-associated SJS episodes (n = 23).
Conclusions: We report the largest outbreak of SJS in children, which was also predominately associated with Mp infection. Mp-associated SJS was associated with a distinct clinical presentation that included less extensive skin disease, an elevated erythrocyte sedimentation rate, and evidence of a preceding respiratory infection.
Copyright © 2015 by the American Academy of Pediatrics.
Figures
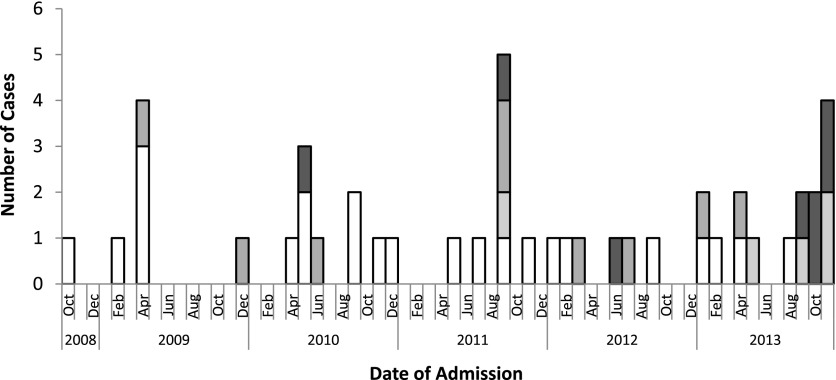
 Confirmed Mp-associated SJS,
Confirmed Mp-associated SJS,  probable Mp-associated SJS,
probable Mp-associated SJS,  possible Mp-associated SJS, and
possible Mp-associated SJS, and  non–Mp-associated SJS.
non–Mp-associated SJS.
References
-
- Stevens AMJ. F. A new eruptive fever associated with stomatitis and ophthalmia: report of two cases in children. Am J Dis Child. 1922;24:526
-
- Atanasković-Marković M, Medjo B, Gavrović-Jankulović M, Ćirković Veličković T, Nikolić D, Nestorović B. Stevens-Johnson syndrome and toxic epidermal necrolysis in children. Pediatr Allergy Immunol. 2013;24(7):645–649 - PubMed
-
- Sekula P, Dunant A, Mockenhaupt M, et al. RegiSCAR study group . Comprehensive survival analysis of a cohort of patients with Stevens-Johnson syndrome and toxic epidermal necrolysis. J Invest Dermatol. 2013;133(5):1197–1204 - PubMed
-
- Singalavanija S, Limpongsanurak W. Stevens-Johnson syndrome in Thai children: a 29-year study. J Med Assoc Thai. 2011;94(suppl 3):S85–S90 - PubMed
-
- Forman R, Koren G, Shear NH. Erythema multiforme, Stevens-Johnson syndrome and toxic epidermal necrolysis in children: a review of 10 years’ experience. Drug Saf. 2002;25(13):965–972 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
