

Variation in Prenatal Diagnosis of Congenital Heart Disease in Infants
- PMID: 26216324
- PMCID: PMC4844533
- DOI: 10.1542/peds.2014-3783
Variation in Prenatal Diagnosis of Congenital Heart Disease in Infants
Abstract
Background and objective: Prenatal diagnosis allows improved perioperative outcomes for fetuses with certain forms of congenital heart disease (CHD). Variability in prenatal diagnosis has been demonstrated in other countries, leading to efforts to improve fetal imaging protocols and access to care, but has not been examined across the United States. The objective was to evaluate national variation in prenatal detection across geographic region and defect type in neonates and infants with CHD undergoing heart surgery.
Methods: Cardiovascular operations performed in patients ≤6 months of age in the United States and included in the Society of Thoracic Surgeons Congenital Heart Surgery Database (2006-2012) were eligible for inclusion. Centers with >15% missing prenatal diagnosis data were excluded from the study. Prenatal diagnosis rates were compared across geographic location of residence and defect type using the χ(2) test.
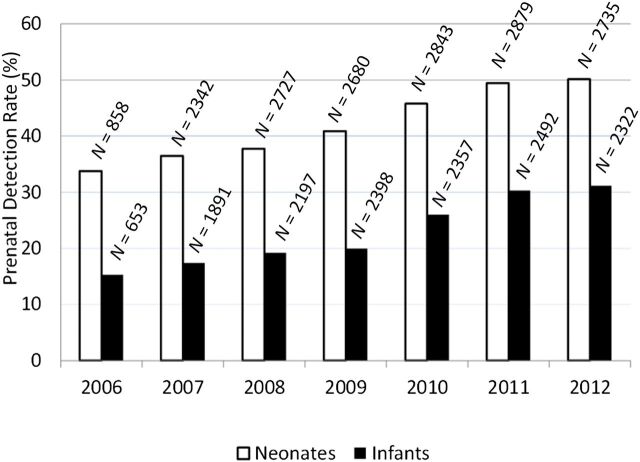
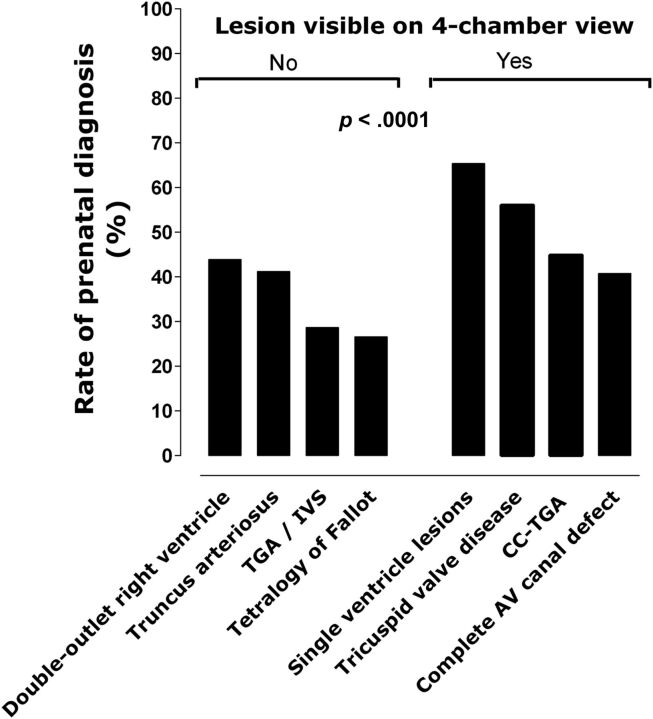
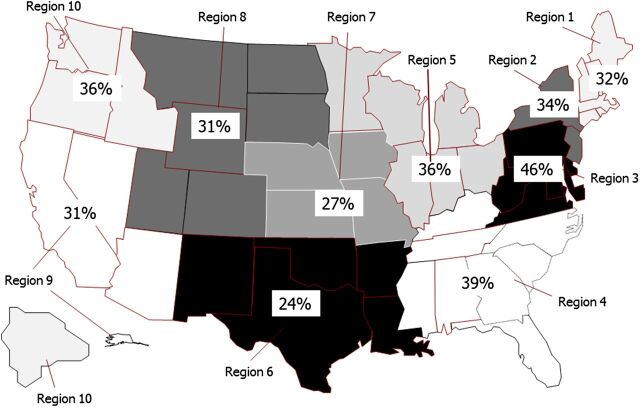
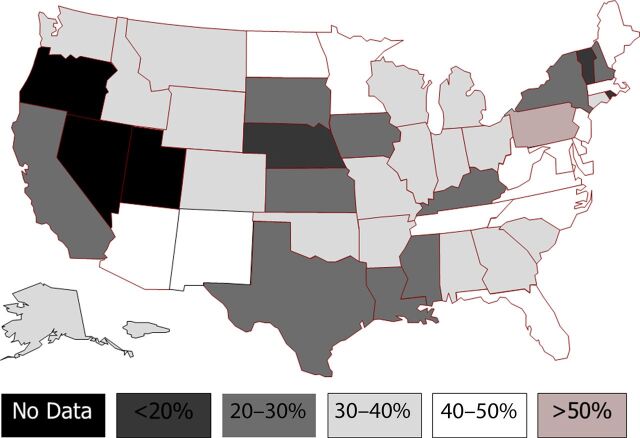
Results: Overall, the study included 31,374 patients from 91 Society of Thoracic Surgeons Congenital Heart Surgery Database participating centers across the United States. Prenatal detection occurred in 34% and increased every year, from 26% (2006) to 42% (2012). There was significant geographic variation in rates of prenatal diagnosis across states (range 11.8%-53.4%, P < .0001). Significant variability by defect type was also observed, with higher rates for lesions identifiable on 4-chamber view than for those requiring outflow tract visualization (57% vs 32%, P < .0001).
Conclusions: Rates of prenatal CHD detection in the United States remain low for patients undergoing surgical intervention, with significant variability between states and across defect type. Additional studies are needed to identify reasons for this variation and the potential impact on patient outcomes.
Copyright © 2015 by the American Academy of Pediatrics.
Conflict of interest statement
Figures
References
-
- Ferencz C , Rubin JD , McCarter RJ , et al. Congenital heart disease: prevalence at livebirth. The Baltimore–Washington Infant Study. Am J Epidemiol. 1985;121(1):31–36 - PubMed
-
- Hoffman JI . Incidence of congenital heart disease: II. Prenatal incidence. Pediatr Cardiol. 1995;16(4):155–165 - PubMed
-
- Talner CN . Report of the New England Regional Infant Cardiac Program, by Donald C. Fyler, MD, Pediatrics, 1980;65(suppl):375–461. Pediatrics. 1998;102(1 pt 2):258–259 - PubMed
-
- Tworetzky W , McElhinney DB , Reddy VM , Brook MM , Hanley FL , Silverman NH . Improved surgical outcome after fetal diagnosis of hypoplastic left heart syndrome. Circulation. 2001;103(9):1269–1273 - PubMed
-
- Bonnet D , Coltri A , Butera G , et al. Detection of transposition of the great arteries in fetuses reduces neonatal morbidity and mortality. Circulation. 1999;99(7):916–918 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
