

IOP telemetry in the nonhuman primate
- PMID: 26216571
- PMCID: PMC5576718
- DOI: 10.1016/j.exer.2015.07.015
IOP telemetry in the nonhuman primate
Abstract
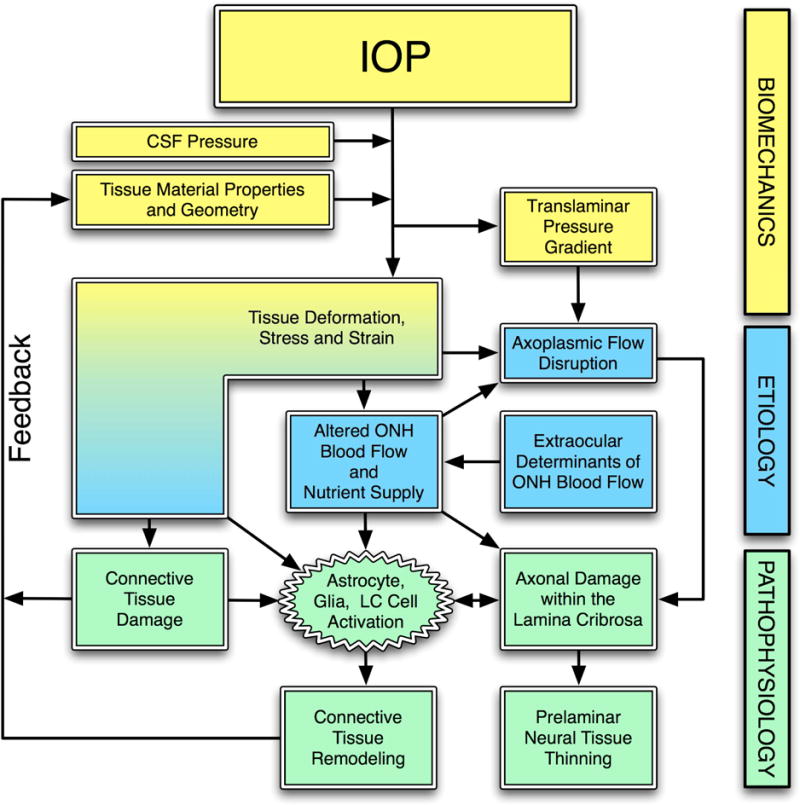
This review is focused on continuous IOP monitoring using telemetry systems in the nonhuman primate (NHP), presented in the context that IOP fluctuations at various timescales may be involved in glaucoma pathogenesis and progression. We use glaucoma as the primary framework to discuss how the dynamic nature of IOP might change with age, racial heritage, and disease in the context of glaucoma susceptibility and progression. We focus on the limited work that has been published in IOP telemetry in NHPs, as well as the emerging data and approaches. We review the ongoing efforts to measure continuous IOP, and the strengths, weaknesses and general pitfalls of the various approaches.
Keywords: Biomechanics; Glaucoma; IOP; Nonhuman primate; Telemetry.
Copyright © 2015 Elsevier Ltd. All rights reserved.
Figures
References
-
- The Advanced Glaucoma Intervention Study (AGIS): 7. The relationship between control of intraocular pressure and visual field deterioration. The AGIS Investigators. Am J Ophthalmol. 2000;130(4):429–440. - PubMed
-
- The Advanced Glaucoma Intervention Study (AGIS): 12. Baseline risk factors for sustained loss of visual field and visual acuity in patients with advanced glaucoma. Am J Ophthalmol. 2002;134(4):499–512. - PubMed
-
- Bengtsson B, Heijl A. Diurnal IOP fluctuation: not an independent risk factor for glaucomatous visual field loss in high-risk ocular hypertension. Graefes Arch Clin Exp Ophthalmol. 2005;243(6):513–518. - PubMed
-
- Bengtsson B, Leske MC, Hyman L, Heijl A. Fluctuation of intraocular pressure and glaucoma progression in the early manifest glaucoma trial. Ophthalmology. 2007;114(2):205–209. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
