

Endoscopic and clinical evaluation of treatment and prognosis of Cronkhite-Canada syndrome: a Japanese nationwide survey
- PMID: 26216651
- PMCID: PMC4805704
- DOI: 10.1007/s00535-015-1107-7
Endoscopic and clinical evaluation of treatment and prognosis of Cronkhite-Canada syndrome: a Japanese nationwide survey
Abstract
Background: First reported in 1955, Cronkhite-Canada syndrome (CCS), a rare syndrome characterized by ectodermal abnormalities and inflammatory changes of the gastrointestinal tract mucosa, has been associated with a poor prognosis and life-threatening malignant complications. In a large population survey, we endeavored to characterize the course and treatment outcome of CCS through clinical and endoscopic assessment, and to explore its optimal treatment and surveillance strategy.
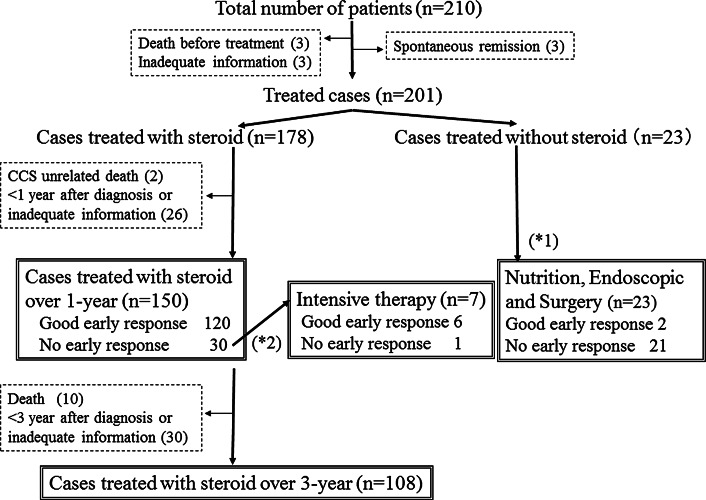
Methods: A retrospective analysis of 210 patients with CCS was conducted via a questionnaire-based nationwide survey of 983 teaching hospitals located throughout Japan. We assessed clinical features, endoscopic findings, treatments used, and short- and long-term outcomes.
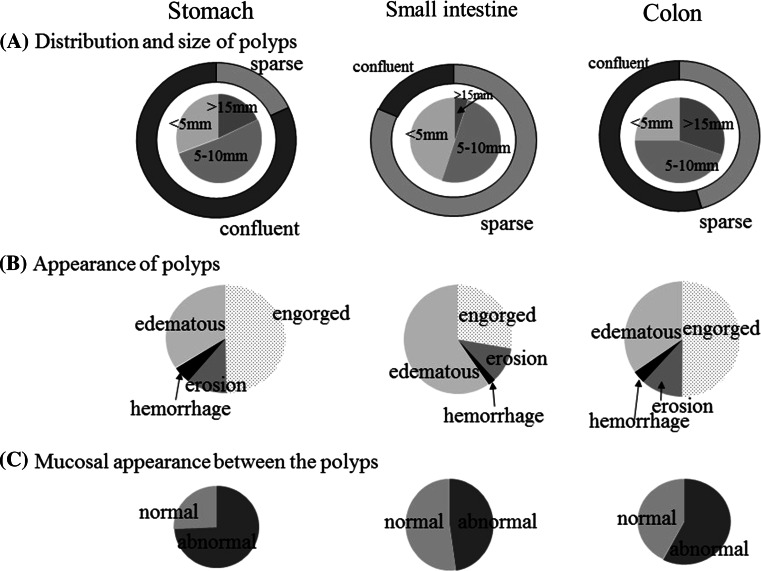
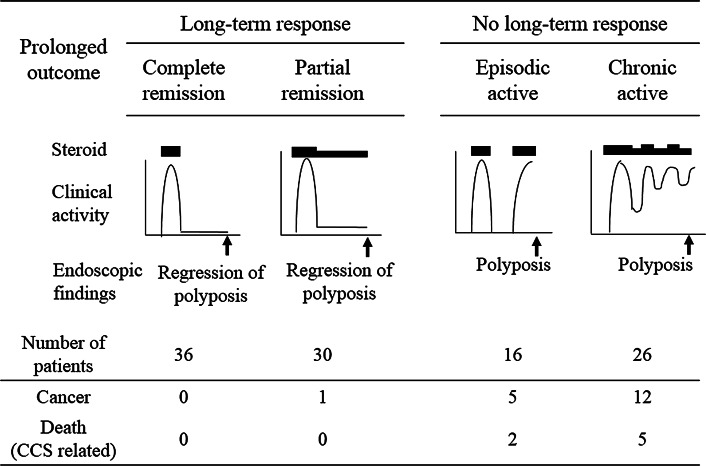
Results: The average age at diagnosis was 63.5 years. In all cases, upper or lower gastrointestinal tract polyposis was confirmed, accompanied by characteristic ectodermal abnormalities. Of the treatments used, oral corticosteroids (30-49 mg/day) were the most effective treatment for active disease, with adjunctive nutritional support considered beneficial. With corticosteroid treatment, abdominal symptoms were relieved within a few months, whereas polyp regression often required more than 6 months. Maintenance of endoscopic remission with or without steroids for 3 years significantly lowered the development of CCS-related cancer, compared with relapsers or nonresponders, underscoring the importance of sustained endoscopic remission for cancer prevention.
Conclusions: The prognosis of CCS has greatly improved through the use of improved medical treatment. Although CCS continues to be relentlessly progressive, carrying a high cancer risk, a sufficient dose and duration of corticosteroid therapy accompanied by nutritional support and periodic endoscopic surveillance appears to improve its natural history.
Keywords: Acquired gastrointestinal polyposis syndrome; Colon cancer; Gastric cancer; Malnutrition.
Figures

Comment in
-
Dermoscopic and histological findings in Cronkhite-Canada syndrome: a report of two cases.Int J Dermatol. 2023 Mar;62(3):e196-e199. doi: 10.1111/ijd.16443. Epub 2022 Oct 2. Int J Dermatol. 2023. PMID: 36183299 No abstract available.
Similar articles
-
The challenging diagnosis of Cronkhite-Canada syndrome in the upper gastrointestinal tract: a series of 7 cases with clinical follow-up.Am J Surg Pathol. 2014 Feb;38(2):215-23. doi: 10.1097/PAS.0000000000000098. Am J Surg Pathol. 2014. PMID: 24418855
-
The Long-Term Clinical and Endoscopic Outcomes of Cronkhite-Canada Syndrome.Clin Transl Gastroenterol. 2020 Apr;11(4):e00167. doi: 10.14309/ctg.0000000000000167. Clin Transl Gastroenterol. 2020. PMID: 32352683 Free PMC article.
-
Cronkhite-Canada syndrome with esophagus involvement and six-year follow-up: A case report.World J Gastroenterol. 2024 Feb 28;30(8):984-990. doi: 10.3748/wjg.v30.i8.984. World J Gastroenterol. 2024. PMID: 38516236 Free PMC article.
-
A severe course of Cronkhite-Canada syndrome and the review of clinical features and therapy in 49 Chinese patients.Turk J Gastroenterol. 2013;24(3):277-85. doi: 10.4318/tjg.2013.0527. Turk J Gastroenterol. 2013. PMID: 24226722 Review.
-
Cronkhite-Canada syndrome: A case report and literature review.Medicine (Baltimore). 2024 Oct 25;103(43):e40242. doi: 10.1097/MD.0000000000040242. Medicine (Baltimore). 2024. PMID: 39470508 Free PMC article. Review.
Cited by
-
Cronkhite-Canada syndrome with steroid dependency: A case report.World J Clin Cases. 2021 May 16;9(14):3466-3471. doi: 10.12998/wjcc.v9.i14.3466. World J Clin Cases. 2021. PMID: 34002159 Free PMC article.
-
Comprehensive treatment and a rare presentation of Cronkhite-Canada syndrome: Two case reports and review of literature.World J Gastrointest Surg. 2023 Nov 27;15(11):2646-2656. doi: 10.4240/wjgs.v15.i11.2646. World J Gastrointest Surg. 2023. PMID: 38111781 Free PMC article.
-
The first report on effect of fecal microbiota transplantation as a complementary treatment in a patient with steroid-refractory Cronkhite-Canada syndrome: A case report.Medicine (Baltimore). 2022 Mar 25;101(12):e29135. doi: 10.1097/MD.0000000000029135. Medicine (Baltimore). 2022. PMID: 35357354 Free PMC article.
-
Cronkhite-Canada syndrome: treatment responses and improved overall survival.Int J Colorectal Dis. 2023 Feb 13;38(1):39. doi: 10.1007/s00384-023-04332-w. Int J Colorectal Dis. 2023. PMID: 36781513
-
Cronkhite-Canada Syndrome Associated with Metastatic Colon Cancer.Case Rep Gastroenterol. 2018 Apr 13;12(1):109-115. doi: 10.1159/000479220. eCollection 2018 Jan-Apr. Case Rep Gastroenterol. 2018. PMID: 29805353 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
