

Self-perceived vs actual and desired weight and body mass index in adult ambulatory general internal medicine patients: a cross sectional study
- PMID: 26217512
- PMCID: PMC4511430
- DOI: 10.1186/s40608-014-0026-0
Self-perceived vs actual and desired weight and body mass index in adult ambulatory general internal medicine patients: a cross sectional study
Abstract
Background: No study has compared patients' self-reported heights and weights (and resultant self-reported body mass indexes [BMIs]) with their actual heights, weights, and BMIs; their self-perceived BMI categories; and their desired weights and BMIs and determined rates of clinicians' documented diagnoses of overweight and obesity in affected patients in a single patient group. The objectives of this study were to make these comparisons, determine patient factors associated with accurate self-perceived BMI categorization, and determine the frequency of clinicians' documented diagnoses of overweight and obesity in affected patients.
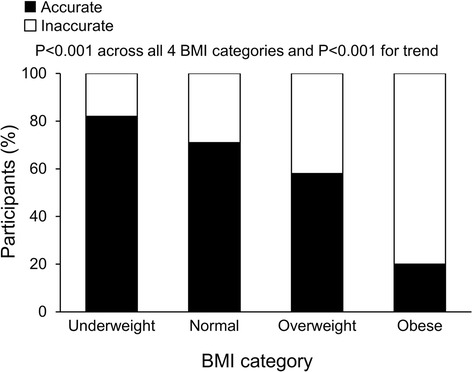
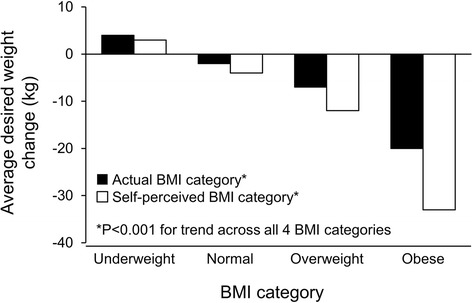
Results: A total of 508 consecutive adult general internal medicine outpatients (257 women, 251 men; mean age, 62.9 ± 14.9 years) seen at Mayo Clinic in Rochester, Minnesota, between November 9 and 20, 2009, completed a questionnaire in which they reported their heights, weights, self-perceived BMI categories ("underweight," "about right," "overweight," or "obese"), and desired weights. These self-reported data were compared to actual heights, actual weights, and actual BMI categories (measured after the questionnaire was completed). Overall, 70% of the patients were overweight or obese. The average self-reported weight was significantly lower than the average actual weight (80.3 ± 20.1 kg vs 81.9 ± 21.1 kg; P < .001). The average self-reported BMI was significantly lower than the average actual BMI (27.6 ± 5.7 kg/m(2) vs 28.3 ± 6.1 kg/m(2); P < .001). Overall, 32% of patients had obesity; however, only 6% perceived they were obese. Accuracy of self-perceived BMI category decreased with higher actual BMI category (P < .001 for trend). Female sex, higher education level, smoking status, and lower BMI were associated with higher accuracy of self-perceived BMI category. Desired weight loss increased with higher self-perceived and actual BMI categories (P < .001 for trends). Of the 165 patients who actually were obese, only 40 (24%) had obesity documented as a diagnosis in their medical records by their clinicians. Statistical tests used were the paired t test, the Pearson χ2 test, the Cochrane-Armitage trend test, the Wald test of marginal homogeneity, analysis of variance, and univariate and multivariate logistic regression.
Conclusions: Many obese patients inaccurately perceive their BMI categories; accuracy decreases with increasing BMI. Clinicians should inform patients of their BMIs and prescribe treatment plans for those with overweight and obesity.
Keywords: Body mass index; Diagnosis; Obesity; Overweight; Patient education.
Figures
Similar articles
-
Do acute hospitalised patients in Australia have a different body mass index to the general Australian population: a point prevalence study?Aust Health Rev. 2018 Apr;42(2):121-129. doi: 10.1071/AH16171. Aust Health Rev. 2018. PMID: 28225703
-
Differential perceptions of body image and body weight among adults of different socioeconomic status in a sub-urban population.J Biosoc Sci. 2014 May;46(3):279-93. doi: 10.1017/S002193201300028X. Epub 2013 May 31. J Biosoc Sci. 2014. PMID: 23721833
-
Comparison of self-perceived weight and desired weight versus actual body mass index among adolescents in Jamaica.Rev Panam Salud Publica. 2011 Apr;29(4):267-76. doi: 10.1590/s1020-49892011000400008. Rev Panam Salud Publica. 2011. PMID: 21603772
-
Increased body mass index and adjusted mortality in ICU patients with sepsis or septic shock: a systematic review and meta-analysis.Crit Care. 2016 Jun 15;20(1):181. doi: 10.1186/s13054-016-1360-z. Crit Care. 2016. PMID: 27306751 Free PMC article.
-
Misclassification of Self-Reported Body Mass Index Categories.Dtsch Arztebl Int. 2020 Apr 10;117(15):253-260. doi: 10.3238/arztebl.2020.0253. Dtsch Arztebl Int. 2020. PMID: 32449888 Free PMC article.
Cited by
-
An Analysis of Real, Self-Perceived, and Desired BMI: Is There a Need for Regular Screening to Correct Misperceptions and Motivate Weight Reduction?Front Public Health. 2017 Feb 8;5:12. doi: 10.3389/fpubh.2017.00012. eCollection 2017. Front Public Health. 2017. PMID: 28229069 Free PMC article.
-
How long do people stick to a diet resolution? A digital epidemiological estimation of weight loss diet persistence.Public Health Nutr. 2020 Dec;23(18):3257-3268. doi: 10.1017/S1368980020001597. Public Health Nutr. 2020. PMID: 33308350 Free PMC article.
-
Current perspective for tube feeding in the elderly: from identifying malnutrition to providing of enteral nutrition.Clin Interv Aging. 2018 Aug 1;13:1353-1364. doi: 10.2147/CIA.S134919. eCollection 2018. Clin Interv Aging. 2018. PMID: 30122907 Free PMC article. Review.
-
Community BMI Surveillance Using an Existing Immunization Registry in San Diego, California.J Community Health. 2017 Jun;42(3):558-564. doi: 10.1007/s10900-016-0288-1. J Community Health. 2017. PMID: 27837356
-
Perception of a need to change weight in individuals living with and beyond breast, prostate and colorectal cancer: a cross-sectional survey.J Cancer Surviv. 2024 Jun;18(3):844-853. doi: 10.1007/s11764-023-01333-0. Epub 2023 Jan 26. J Cancer Surviv. 2024. PMID: 36701100 Free PMC article.
References
-
- AMA Newsroom Room: AMA adopts new policies on second day of voting at annual meeting: obesity as a disease [www.ama-assn.org/ama/pub/news/news/2013/2013-06-18-new-ama-policies-annu...]
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
