

Prevalence of obesity and overweight, its clinical markers and associated factors in a high risk South-Asian population
- PMID: 26217531
- PMCID: PMC4510896
- DOI: 10.1186/s40608-015-0044-6
Prevalence of obesity and overweight, its clinical markers and associated factors in a high risk South-Asian population
Abstract
Background: Obesity is a global epidemic, which is a risk factor for cardiovascular diseases and metabolic abnormalities. It is measured by body mass index (BMI), waist circumference (WC), waist-hip ratio (WHR), body fat (BF) distribution and abdominal fat mass, each having its own merits and limitations. Variability in body composition between ethnic groups in South-Asians is significant and may not be truly reflected by BMI alone, which may result in misclassification. This study therefore, aims to determine the frequency of obesity, body fat composition and distribution, in a high risk population of an urban slum of Karachi, Pakistan. This survey included 451 participants selected by systematic sampling who were administered pre-tested questionnaires on socio-demographics, diet and physical activity. Chi-square was used to determine the association between categorical variables and multiple linear regression was used for quantitative variables. A P value of less than 0.05 was considered significant.
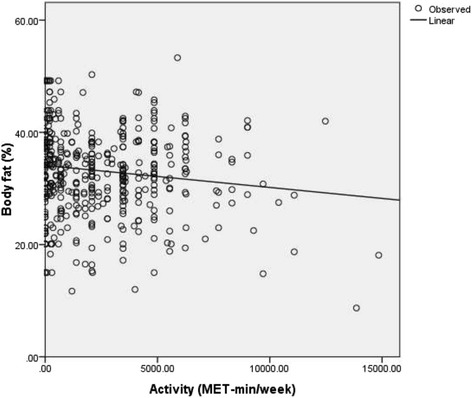
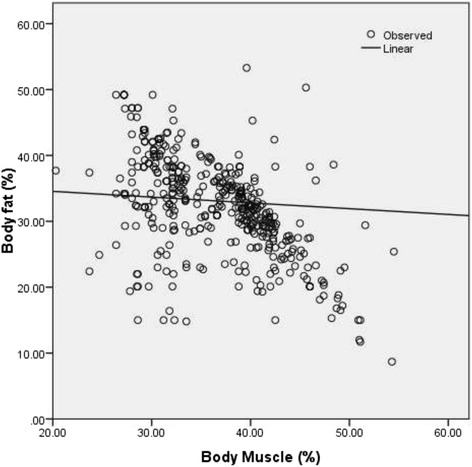
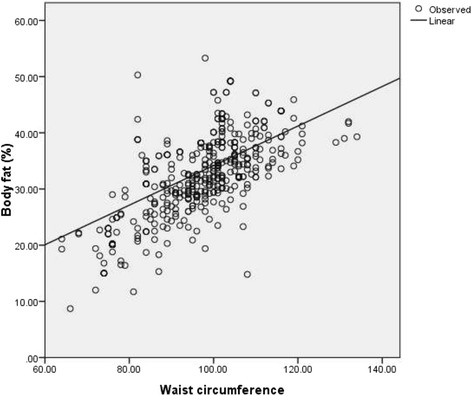
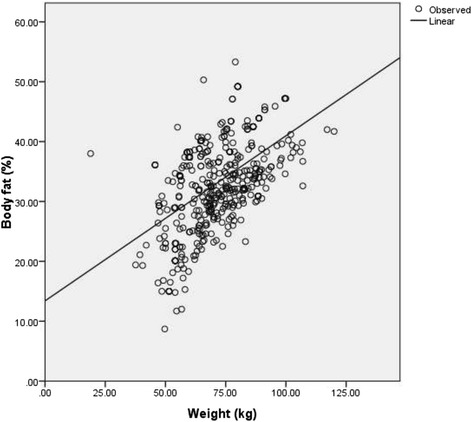
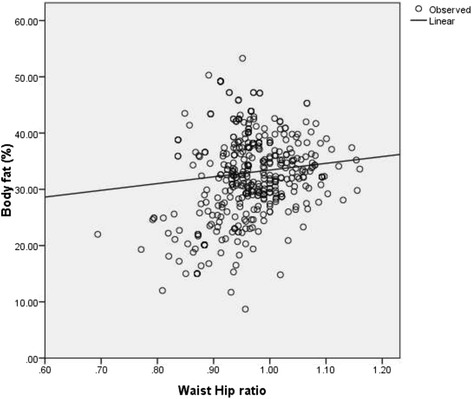
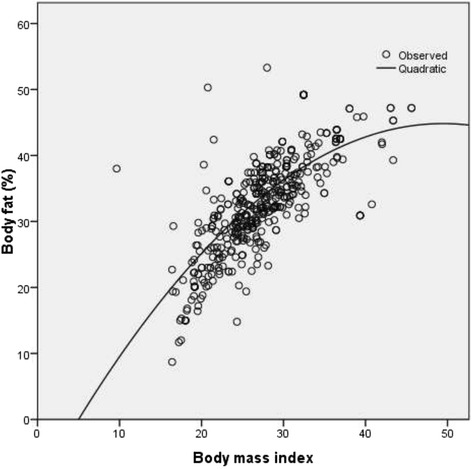
Results: Classified by BMI, 29% study subjects were overweight and 21% obese (58.7% with central obesity). Body fat percent (BF%) classified 81% as overweight. Females were more obese (P 0.03) with higher prevalence of central obesity (P <0.001) and WHR (P 0.003) but with a lower muscle mass (P 0.001). Activity score and muscle mass showed inverse linear association with BF% whereas, WC, weight, BMI and WHR had a positive linear association with BF%. The relationship between BMI and BF% was quadratic with a weaker association at lower BMI. Adjusting for socio-demographic variables, BF%, weight, diastolic blood pressure (DBP), BMI and score on the diet questionnaire had a positive linear association with WC, while WC, WHR and BP had a positive linear association with BF%. BF%, muscle content and WC had a positive linear association with BMI.
Conclusion: Considering lower cut-offs for South-Asians BMI and WC, this study showed a high prevalence of obesity among a sub-urban population of Karachi, which was even higher when BF% was measured. Considering the rising prevalence of non-communicable diseases, BF%, WC, WHR and BMI measurements are convenient and feasible means of identifying population at risk and hence addressing it through public awareness and early detection.
Keywords: Body fat percentage; Body mass index; Obesity; Waist circumference; Waist-hip ratio.
Figures
Similar articles
-
Validity of simple, novel measures of generalized and central obesity among young Asian Indian women.Indian J Med Sci. 2011 Dec;65(12):518-27. Indian J Med Sci. 2011. PMID: 23548252
-
Does body mass index reflect adequately the body fat content in perimenopausal women?Maturitas. 2005 Jul 16;51(3):307-13. doi: 10.1016/j.maturitas.2004.08.014. Maturitas. 2005. PMID: 15978975
-
[Association of obesity indexes with hypertension and dyslipidemia in Chinese adults].Wei Sheng Yan Jiu. 2018 Nov;47(6):875-882. Wei Sheng Yan Jiu. 2018. PMID: 30593325 Chinese.
-
Overview of epidemiology and contribution of obesity to cardiovascular disease.Prog Cardiovasc Dis. 2014 Jan-Feb;56(4):369-81. doi: 10.1016/j.pcad.2013.10.016. Epub 2013 Oct 24. Prog Cardiovasc Dis. 2014. PMID: 24438728 Review.
-
Salivary Leptin Level in Young Adult Males and its Association with Anthropometric Measurements, Fat Distribution and Muscle Mass.Eur Endocrinol. 2018 Sep;14(2):94-98. doi: 10.17925/EE.2018.14.2.94. Epub 2018 Sep 10. Eur Endocrinol. 2018. PMID: 30349601 Free PMC article. Review.
Cited by
-
Current Trends of Cardiovascular Risk Determinants in Pakistan.Cureus. 2018 Oct 4;10(10):e3409. doi: 10.7759/cureus.3409. Cureus. 2018. PMID: 30542628 Free PMC article.
-
Relationship between body mass index and percentage of body fat, estimated by bio-electrical impedance among adult females in a rural community of North India: A cross-sectional study.J Postgrad Med. 2019 Jul-Sep;65(3):134-140. doi: 10.4103/jpgm.JPGM_218_18. J Postgrad Med. 2019. PMID: 31169130 Free PMC article.
-
Individual and community-level determinants of overweight and obesity among urban men: Further analysis of the Ethiopian demographic and health survey.PLoS One. 2021 Nov 4;16(11):e0259412. doi: 10.1371/journal.pone.0259412. eCollection 2021. PLoS One. 2021. PMID: 34735510 Free PMC article.
-
Effects of food price on nutrition outcomes among women in Nigeria.Food Sci Nutr. 2023 Oct 3;12(1):94-104. doi: 10.1002/fsn3.3737. eCollection 2024 Jan. Food Sci Nutr. 2023. PMID: 38268895 Free PMC article.
-
Double Burden of Underweight and Overweight among Women in South and Southeast Asia: A Systematic Review and Meta-analysis.Adv Nutr. 2020 Jan 1;11(1):128-143. doi: 10.1093/advances/nmz078. Adv Nutr. 2020. PMID: 31634389 Free PMC article.
References
-
- Klein S, Allison DB, Heymsfield SB, Kelley DE, Leibel RL, Nonas C, et al. Waist circumference and cardiometabolic risk: a consensus statement from shaping america’s health: association for weight management and obesity prevention; NAASO, the Obesity Society; the American Society for Nutrition; and the American Diabetes Association. Obesity. 2007;15(5):1061–7. doi: 10.1038/oby.2007.632. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
