

Results of Open Surgical Repair of Chronic Juxtarenal Aortic Occlusion
- PMID: 26217622
- PMCID: PMC4480295
- DOI: 10.5758/vsi.2014.30.3.81
Results of Open Surgical Repair of Chronic Juxtarenal Aortic Occlusion
Abstract
Purpose: The aim of study was to review the results of open surgical repair (OSR) of chronic juxtarenal aortic occlusion (JRAO).
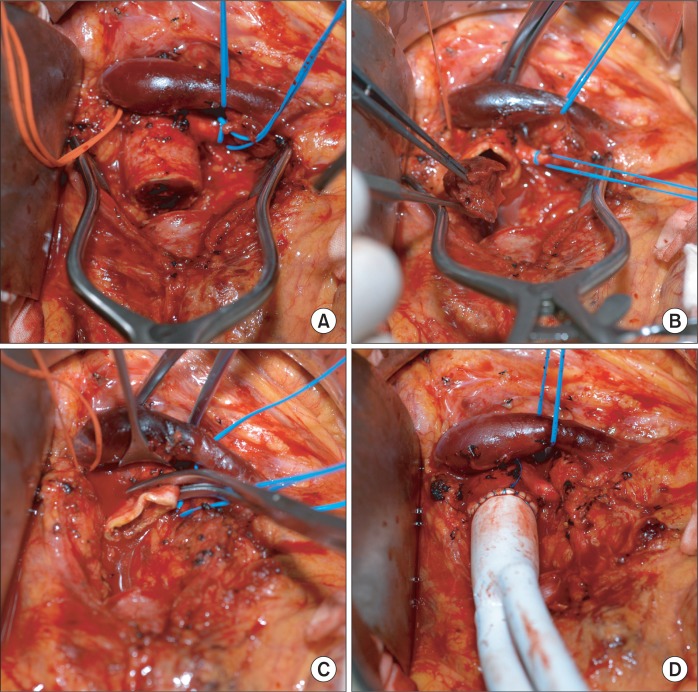
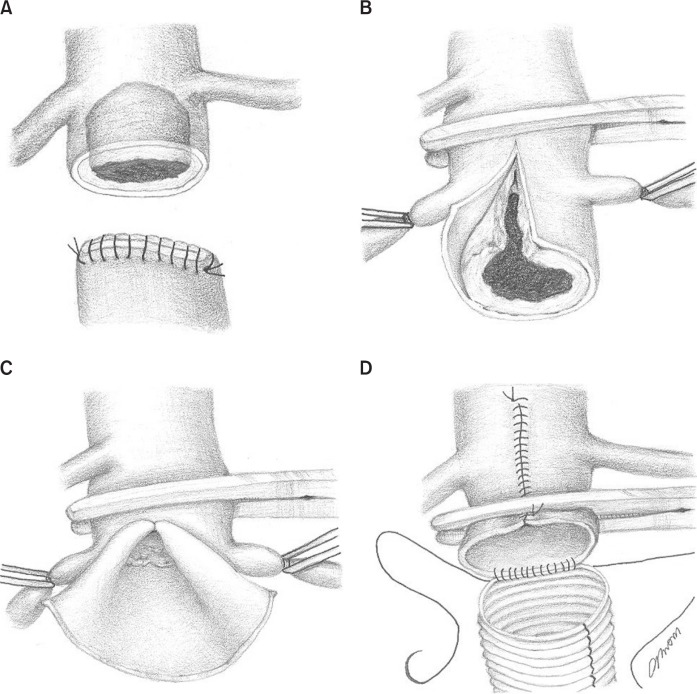
Materials and methods: We retrospectively reviewed the results of OSR performed in 47 patients (male, 92%; mean age, 59.9±9.3 years [range, 44-79]) with chronic JRAO during the past 21 years. In order to reduce intraoperative renal ischemic time (RIT), we excised a portion of the occluded segment of the infrarenal aorta without proximal aortic clamping. We then performed suprarenal aortic clamping with both renal arteries clamped, removed the proximal aortic thrombus cap, confirmed both renal artery orifices, and moved the suprarenal aortic clamp to the infrarenal aorta to allow renal perfusion and standard aortoiliac reconstruction. We investigated early (<30 days) postoperative surgical morbidity (particularly renal function), operative mortality, and longterm patient survival. We conducted risk factor analysis for postoperative renal insufficiency.
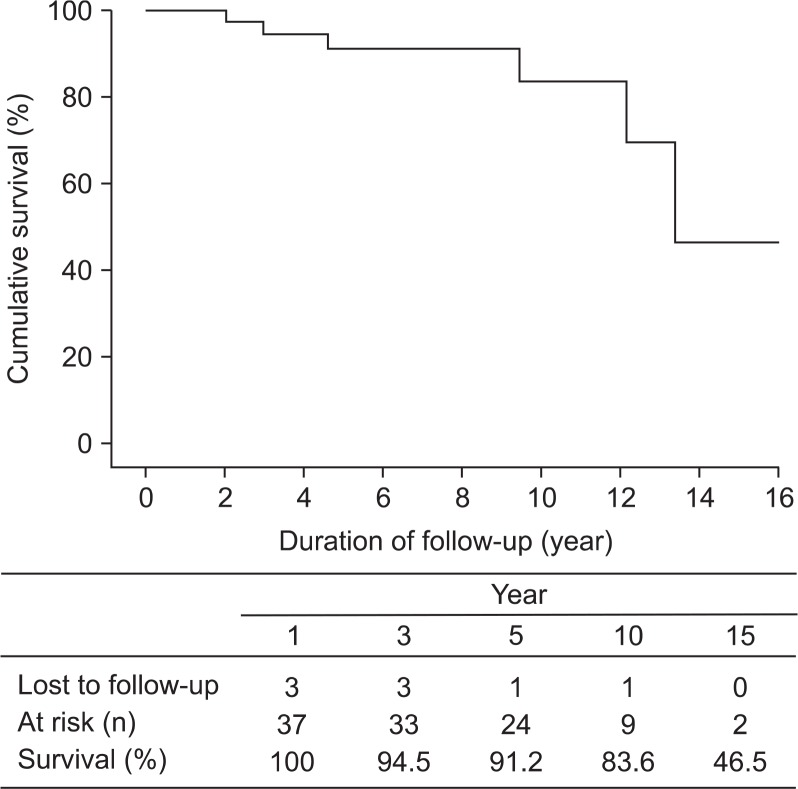
Results: The mean intraoperative RIT was 10.7±5.5 minutes (range, 3-25), including 6 patients who underwent concomitant pararenal aortic thromboendarterectomy. Postoperatively, five (11%) patients had transient renal insufficiency, one had pneumonia, and one patient had an acute myocardial infarction. However, there was no operative mortality or newly developed dialysis-dependent renal failure. Postoperative follow up was available in 36 (77%) patients for a mean period of 6.3 years (range, 1 month-17 years). Kaplan Meier calculations of patient survival at 5 and 10 years after surgery were 91.2% and 83.6%, respectively.
Conclusion: We have experienced short RIT, acceptable early postoperative results and long-term survival after OSR of chronic JRAO.
Keywords: Juxtarenal aortic occlusion; Renal complication; Renal ischemic time; Surgical results.
Figures
Similar articles
-
Experiences of Surgical Treatment for Juxtarenal Aortic Occlusion.Vasc Specialist Int. 2014 Mar;30(1):19-25. doi: 10.5758/vsi.2014.30.1.19. Epub 2014 Mar 30. Vasc Specialist Int. 2014. PMID: 26217611 Free PMC article.
-
A contemporary experience of open aortic reconstruction in patients with chronic atherosclerotic occlusion of the abdominal aorta.J Vasc Surg. 2010 Nov;52(5):1164-72. doi: 10.1016/j.jvs.2010.05.112. Epub 2010 Aug 21. J Vasc Surg. 2010. PMID: 20732782
-
Editor's Choice - Durability of Open Repair of Juxtarenal Abdominal Aortic Aneurysms: A Multicentre Retrospective Study in Five French Academic Centres.Eur J Vasc Endovasc Surg. 2020 Jan;59(1):40-49. doi: 10.1016/j.ejvs.2019.05.010. Epub 2019 Sep 14. Eur J Vasc Endovasc Surg. 2020. PMID: 31530501
-
Open repair for juxtarenal aortic aneurysms.J Cardiovasc Surg (Torino). 2013 Feb;54(1 Suppl 1):35-45. J Cardiovasc Surg (Torino). 2013. PMID: 23443588 Review.
-
A systematic review and meta-analysis of endovascular juxtarenal aortic aneurysm repair demonstrates lower perioperative mortality compared with open repair.J Vasc Surg. 2019 Dec;70(6):2054-2064.e3. doi: 10.1016/j.jvs.2019.04.464. Epub 2019 Jul 18. J Vasc Surg. 2019. PMID: 31327612
References
-
- Imparato AM, Kim GE, Davidson T, Crowley JG. Intermittent claudication: its natural course. Surgery. 1975;78:795–799. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
