

Progressive Resistance Exercise with Eccentric Loading for the Management of Knee Osteoarthritis
- PMID: 26217665
- PMCID: PMC4497310
- DOI: 10.3389/fmed.2015.00045
Progressive Resistance Exercise with Eccentric Loading for the Management of Knee Osteoarthritis
Abstract
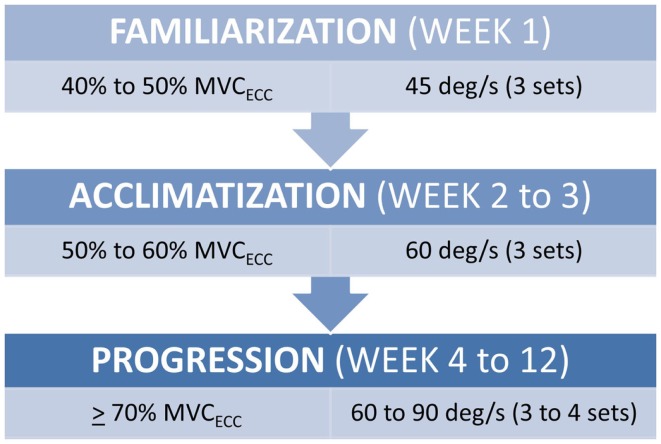
Introduction: The patient was a 58-year-old African-American male with radiographic evidence of bilateral knee osteoarthritis (OA). He participated in a standardized 12-week eccentric strengthening program within a Veterans Affairs (VA) medical center.
Background: The use of an eccentric training paradigm may prove to be beneficial for older adults with knee OA since eccentric muscle actions are involved in the energy absorption at the knee joint during gait and controlled movement during stair descent. Furthermore, in comparison to standard muscle actions, eccentric muscle actions result in higher torque generation and a lower rate of oxygen consumption at a given level of perceived exertion. Therefore, this mode of progressive resistance exercise may be ideal for older adults.
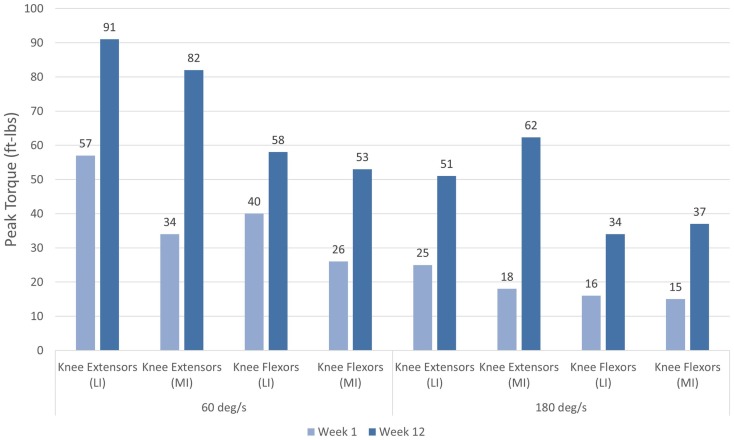
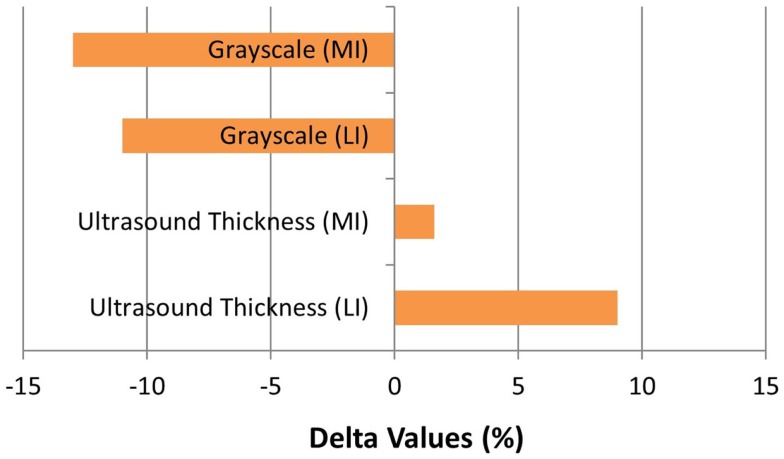
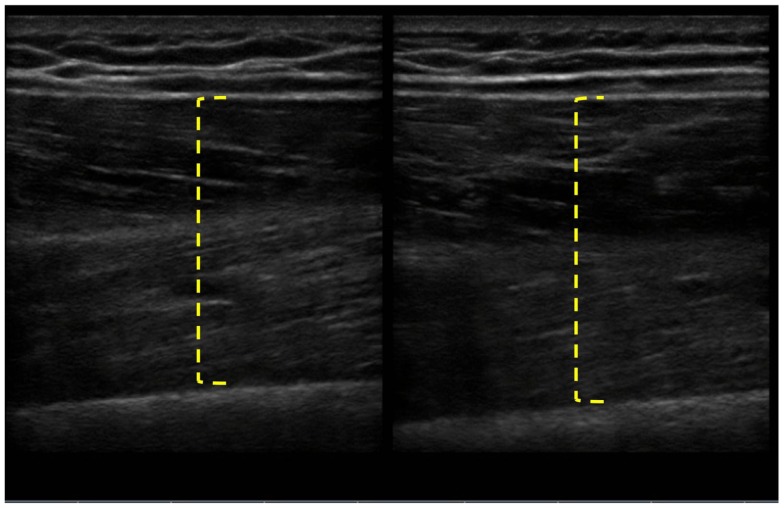
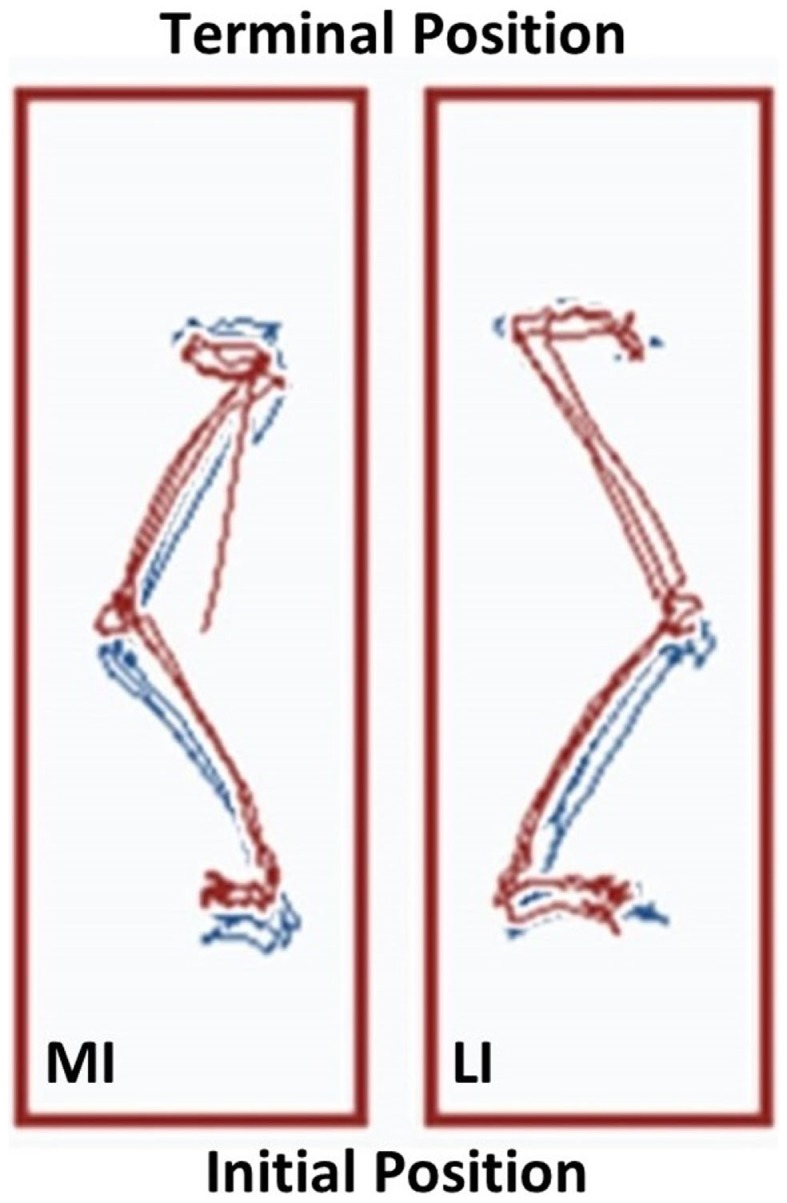
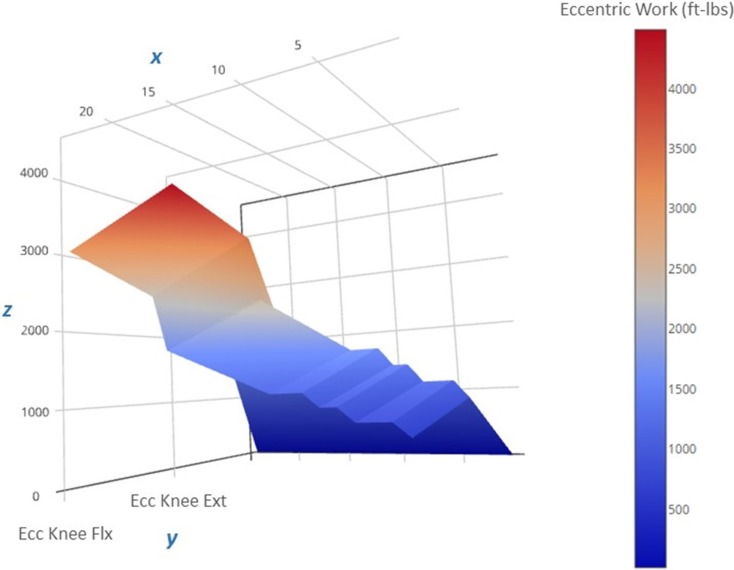
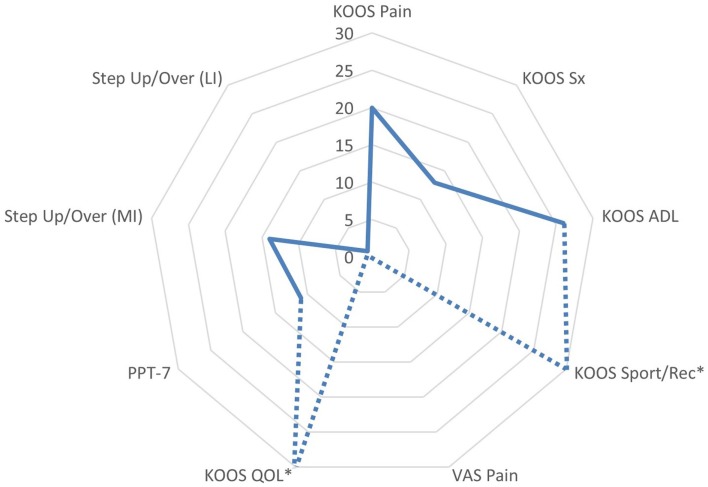
Discussion: The patient completed an eccentric strengthening regimen for the knee flexors and extensors twice per week without an exacerbation of knee pain. Muscle morphology measures of the rectus femoris were measured using diagnostic ultrasound. Isokinetic measures of muscle peak torque were obtained at 60°/s and 180°/s. Functional performance was assessed using a physical performance battery and stair-step performance was assessed from the linear displacement of the center of gravity trajectories obtained with a force plate. Visual analog scale pain ratings and self-reported global disease status were also documented. Post-exercise assessments revealed improvements in sonographic muscle size and tissue composition estimates, peak knee extensor torque (ranging from 60 to 253%), functional performance, and global disease status.
Concluding remarks: The patient exhibited improvements in muscle morphology, muscle strength, functional performance, pain, and global disease status after 12 weeks of an eccentric strengthening regimen. The intervention and outcomes featured in this case were feasible to implement within a VA medical center and merit further investigation.
Keywords: eccentric exercise; knee arthritis; strengthening; ultrasound; veterans.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases