

Clinical Epidemiology of Extubation Failure in the Pediatric Cardiac ICU: A Report From the Pediatric Cardiac Critical Care Consortium
- PMID: 26218260
- PMCID: PMC4672991
- DOI: 10.1097/PCC.0000000000000498
Clinical Epidemiology of Extubation Failure in the Pediatric Cardiac ICU: A Report From the Pediatric Cardiac Critical Care Consortium
Abstract
Objective: To describe the clinical epidemiology of extubation failure in a multicenter cohort of patients treated in pediatric cardiac ICUs.
Design: Retrospective cohort study using prospectively collected clinical registry data.
Setting: Pediatric Cardiac Critical Care Consortium registry.
Patients: All patients admitted to the CICU at Pediatric Cardiac Critical Care Consortium hospitals.
Interventions: None.
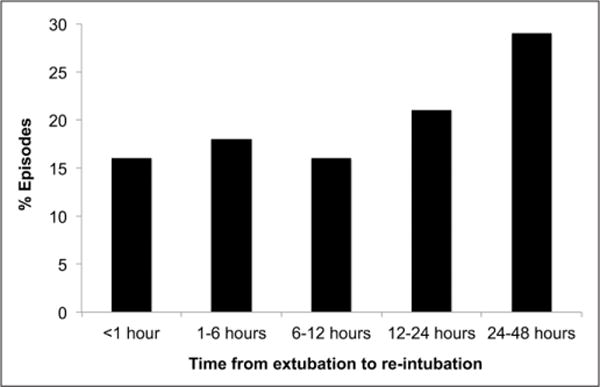
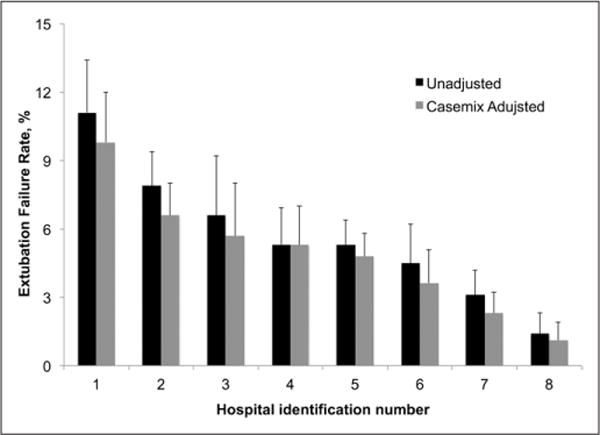
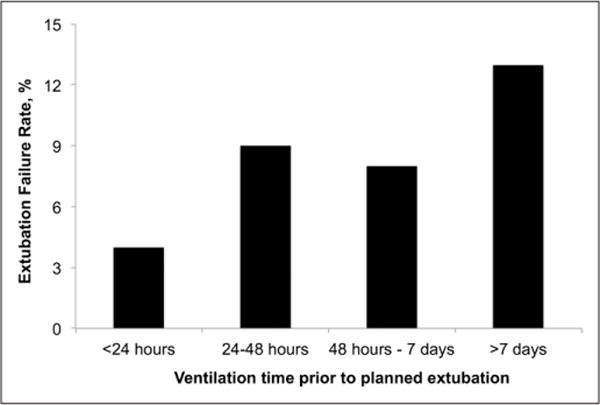
Measurements and main results: Analysis of all mechanical ventilation episodes in the registry from October 1, 2013, to July 31, 2014. The primary outcome of extubation failure was reintubation less than 48 hours after planned extubation. Repeated-measures analysis using generalized estimating equations to account for within patient and center correlation was performed to identify risk factors for extubation failure. Adjusted extubation failure rates for each hospital were calculated using logistic regression controlling for patient factors. Of 1,734 mechanical ventilation episodes (1,478 patients at eight hospitals) ending in a planned extubation, there were 100 extubation failures (5.8%). In multivariable analysis, only longer duration of mechanical ventilation was significantly associated with extubation failure (p = 0.01); the failure rate was 4% when ventilated less than 24 hours, 9% after 24 hours, and 13% after 7 days. For 503 patients intubated and extubated in the cardiac operating room, 15 patients (3%) failed extubation within 48 hours (12 within 24 hr). Case-mix-adjusted extubation failure rates ranged from 1.1% to 9.8% across hospitals. Patients failing extubation had greater median cardiac ICU length of stay (15 vs 3 d; p < 0.001) and in-hospital mortality (7.9 vs 1.2%; p < 0.001).
Conclusions: Though extubation failure is uncommon overall, there may be opportunities to improve extubation readiness assessment in patients ventilated more than 24 hours. These data suggest that extubation in the operating room after cardiac surgery can be done with a low failure rate. We observed variation in extubation failure rates across hospitals, and future investigation must elucidate the optimal strategies of high-performing centers to reduce ventilation time while limiting extubation failures.
Conflict of interest statement
Dr. Gaies receives support from the National Heart, Lung, and Blood Institute (K08HL116639, Principal Investigator) that indirectly supports this research. Dr. Gaies received support for article research from the National Institutes of Health (NIH). His institution received grant support from the NIH (K08 award from NHLBI [PI: Gaies]). Dr. Shekerdemian disclosed other support from Pediatric Research (Editorial Board Honorarium, $125 for 2014). Dr. Thiagarajan’s institution consulted for Bristol Myers Squibb (Events Adjudication Committee). Dr. Pasquali’s institution received grant support from the NHLBI and the Children’s Heart Foundation. Dr. Cooper lectured for Cadence and MedImmune and provided expert testimony for Keith L Davidson Law Offices. His institution received grant support from Grifols. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
Comment in
-
Failed Extubation in Cardiac Patients: Not Just Case-Mix and Beware of Slow Progression.Pediatr Crit Care Med. 2015 Nov;16(9):883-4. doi: 10.1097/PCC.0000000000000545. Pediatr Crit Care Med. 2015. PMID: 26536552 No abstract available.
Similar articles
-
Variation in extubation failure rates after neonatal congenital heart surgery across Pediatric Cardiac Critical Care Consortium hospitals.J Thorac Cardiovasc Surg. 2017 Jun;153(6):1519-1526. doi: 10.1016/j.jtcvs.2016.12.042. Epub 2017 Feb 4. J Thorac Cardiovasc Surg. 2017. PMID: 28259455 Free PMC article.
-
Extubation Failure Rates After Pediatric Cardiac Surgery Vary Across Hospitals.Pediatr Crit Care Med. 2019 May;20(5):450-456. doi: 10.1097/PCC.0000000000001877. Pediatr Crit Care Med. 2019. PMID: 30807544 Free PMC article.
-
Risk factors for mechanical ventilation and reintubation after pediatric heart surgery.J Thorac Cardiovasc Surg. 2016 Feb;151(2):451-8.e3. doi: 10.1016/j.jtcvs.2015.09.080. Epub 2015 Sep 28. J Thorac Cardiovasc Surg. 2016. PMID: 26507405
-
Effectiveness of dexmedetomidine versus propofol on extubation times, length of stay and mortality rates in adult cardiac surgery patients: a systematic review and meta-analysis.JBI Database System Rev Implement Rep. 2018 May;16(5):1220-1239. doi: 10.11124/JBISRIR-2017-003488. JBI Database System Rev Implement Rep. 2018. PMID: 29762314
-
Do clinical parameters predict first planned extubation outcome in the pediatric intensive care unit?J Intensive Care Med. 2015 Feb;30(2):89-96. doi: 10.1177/0885066613494338. Epub 2013 Jun 27. J Intensive Care Med. 2015. PMID: 23813884 Review.
Cited by
-
Comparison of high-flow nasal cannula oxygenation and non-invasive ventilation for postoperative pediatric cardiac surgery: a meta-analysis.BMC Pulm Med. 2024 Feb 21;24(1):92. doi: 10.1186/s12890-024-02901-5. BMC Pulm Med. 2024. PMID: 38383357 Free PMC article.
-
Developing an Extubation strategy for the difficult pediatric airway-Who, when, why, where, and how?Paediatr Anaesth. 2022 May;32(5):592-599. doi: 10.1111/pan.14411. Epub 2022 Feb 25. Paediatr Anaesth. 2022. PMID: 35150181 Free PMC article. Review.
-
Nonopioid analgesics for perioperative and cardiac surgery pain in children: Current evidence and knowledge gaps.Ann Pediatr Cardiol. 2020 Jan-Mar;13(1):46-55. doi: 10.4103/apc.APC_190_18. Epub 2019 Dec 4. Ann Pediatr Cardiol. 2020. PMID: 32030035 Free PMC article. Review.
-
Neurally Adjusted Ventilatory Assist Is Associated with Greater Initial Extubation Success in Postoperative Congenital Heart Disease Patients when Compared to Conventional Mechanical Ventilation.J Pediatr Intensive Care. 2018 Sep;7(3):147-158. doi: 10.1055/s-0038-1627099. Epub 2018 Feb 5. J Pediatr Intensive Care. 2018. PMID: 31073487 Free PMC article.
-
Pediatric ventilation weaning.Rev Bras Ter Intensiva. 2020 Jul-Sep;32(3):333-336. doi: 10.5935/0103-507X.20200061. Rev Bras Ter Intensiva. 2020. PMID: 33053022 Free PMC article. No abstract available.
References
-
-
Pediatric Cardiac Critical Care Consortium (PC4). Available at:
http://pc4quality.org . Accessed February 28, 2015
-
-
- Harris KC, Holowachuk S, Pitfield S, et al. Should early extubation be the goal for children after congenital cardiac surgery? J Thorac Cardiovasc Surg. 2014;148:2642–2647. - PubMed
-
- Manrique AM, Feingold B, Di Filippo S, et al. Extubation after cardiothoracic surgery in neonates, children, and young adults: One year of institutional experience. Pediatr Crit Care Med. 2007;8:552–555. - PubMed
-
- Miller JW, Vu D, Chai PJ, et al. Patient and procedural characteristics for successful and failed immediate tracheal extubation in the operating room following cardiac surgery in infancy. Paediatr Anaesth. 2014;24:830–839. - PubMed
-
- Baisch SD, Wheeler WB, Kurachek SC, et al. Extubation failure in pediatric intensive care incidence and outcomes. Pediatr Crit Care Med. 2005;6:312–318. - PubMed
