

A systematic review and meta-analysis of risk factors for postherpetic neuralgia
- PMID: 26218719
- PMCID: PMC4685754
- DOI: 10.1097/j.pain.0000000000000307
A systematic review and meta-analysis of risk factors for postherpetic neuralgia
Abstract
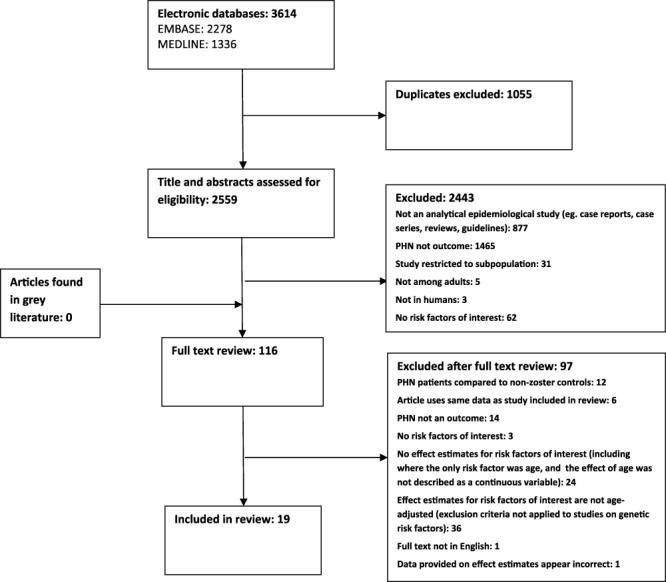
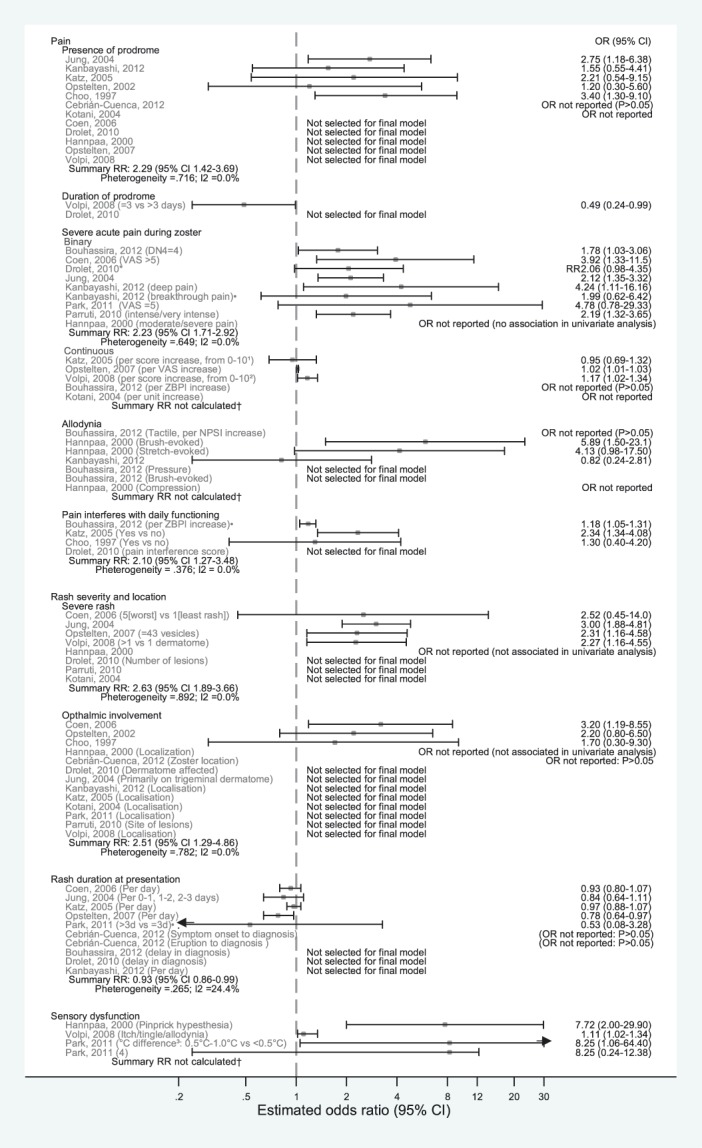
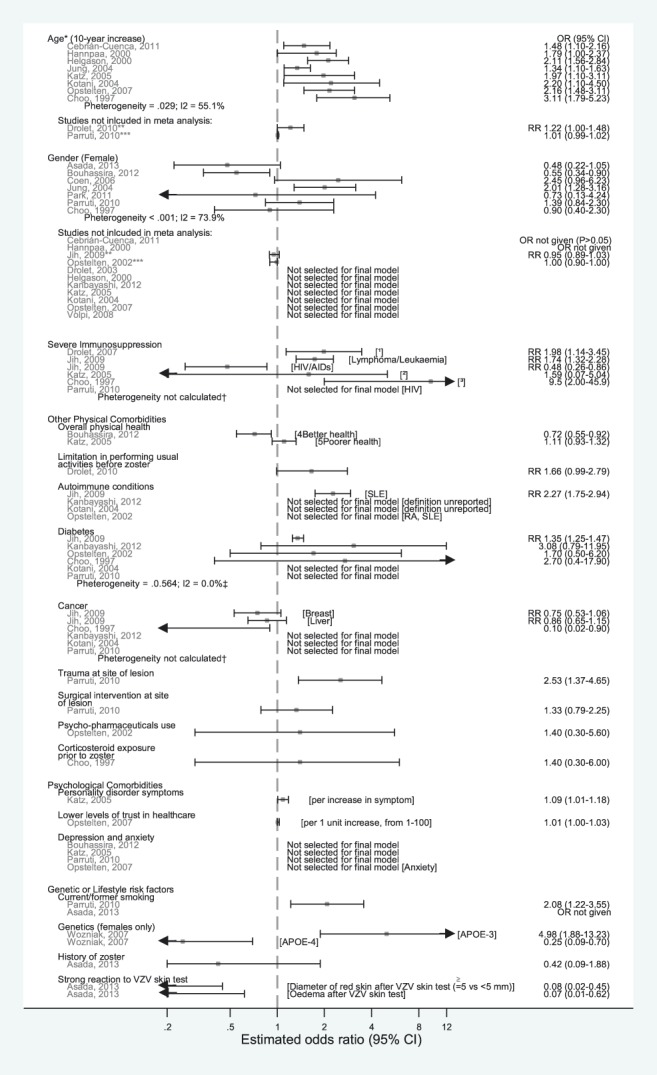
Patients with herpes zoster can develop persistent pain after rash healing, a complication known as postherpetic neuralgia. By preventing zoster through vaccination, the risk of this common complication is reduced. We searched MEDLINE and Embase for studies assessing risk factors for postherpetic neuralgia, with a view to informing vaccination policy. Nineteen prospective studies were identified. Meta-analysis showed significant increases in the risk of postherpetic neuralgia with clinical features of acute zoster including prodromal pain (summary rate ratio 2.29, 95% confidence interval: 1.42-3.69), severe acute pain (2.23, 1.71-2.92), severe rash (2.63, 1.89-3.66), and ophthalmic involvement (2.51, 1.29-4.86). Older age was significantly associated with postherpetic neuralgia; for individual studies, relative risk estimates per 10-year increase ranged from 1.22 to 3.11. Evidence for differences by gender was conflicting, with considerable between-study heterogeneity. A proportion of studies reported an increased risk of postherpetic neuralgia with severe immunosuppression (studies, n = 3/5) and diabetes mellitus (n = 1/4). Systemic lupus erythematosus, recent trauma, and personality disorder symptoms were associated with postherpetic neuralgia in single studies. No evidence of higher postherpetic neuralgia risk was found with depression (n = 4) or cancer (n = 5). Our review confirms a number of clinical features of acute zoster are risk factors for postherpetic neuralgia. It has also identified a range of possible vaccine-targetable risk factors for postherpetic neuralgia; yet aside from age-associated risks, evidence regarding risk factors to inform zoster vaccination policy is currently limited.
Conflict of interest statement
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Figures
References
-
- Asada H, Nagayama K, Okazaki A, Mori Y, Okuno Y, Takao Y, Miyazaki Y, Onishi F, Okeda M, Yano S, Kumihashi H, Gomi Y, Maeda K, Ishikawa T, Iso H, Yamanishi K. An inverse correlation of VZV skin-test reaction, but not antibody, with severity of herpes zoster skin symptoms and zoster-associated pain. J Dermatol Sci 2013;69:243–9. - PubMed
-
- Baron R, Binder A, Wasner G. Neuropathic pain: diagnosis, pathophysiological mechanisms, and treatment. Lancet Neurol 2010;9:807–19. - PubMed
-
- Block AR, Fernandez E, Kremer E. Handbook of pain syndromes. In: Chapter 18-A belt of roses from hell: pain in herpes zoster and postherpetic neuralgia. Psychology Press, Abingdon, United Kingdom: 2013.
-
- Bouhassira D, Chassany O, Gaillat J, Hanslik T, Launay O, Mann C, Rabaud C, Rogeaux O, Strady C. Patient perspective on herpes zoster and its complications: an observational prospective study in patients aged over 50 years in general practice. PAIN 2012;153:342–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
