

Trends in survival for teenagers and young adults with cancer in the UK 1992-2006
- PMID: 26219688
- PMCID: PMC4571927
- DOI: 10.1016/j.ejca.2015.06.112
Trends in survival for teenagers and young adults with cancer in the UK 1992-2006
Abstract
Background: Although relatively rare, cancer in teenagers and young adults (TYA) is the most common disease-related cause of death and makes a major contribution to years of life lost in this age group. There is a growing awareness of the distinctive needs of this age group and drive for greater understanding of how outcomes can be improved. We present here the latest TYA survival trends data for the United Kingdom (UK).
Methods: Using national cancer registry data, we calculated five-year relative survival for all 15-24 year olds diagnosed with cancer or a borderline/benign CNS tumour in the UK during the periods 1992-1996, 1997-2001 and 2002-2006. We analysed trends in survival for all cancers combined and for eighteen specified groups that together represent the majority of TYA cancers. We compared our data with published data for Europe, North America and Australia.
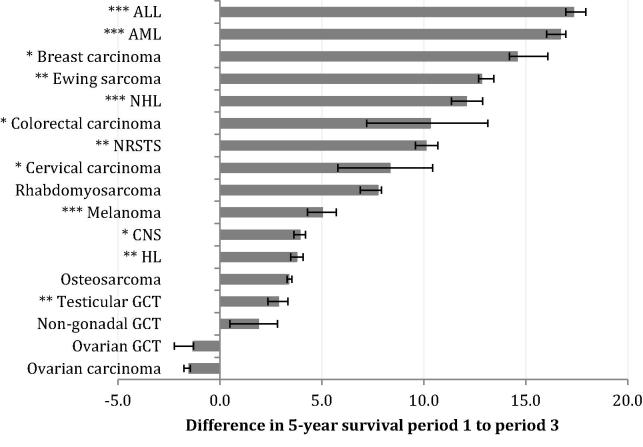
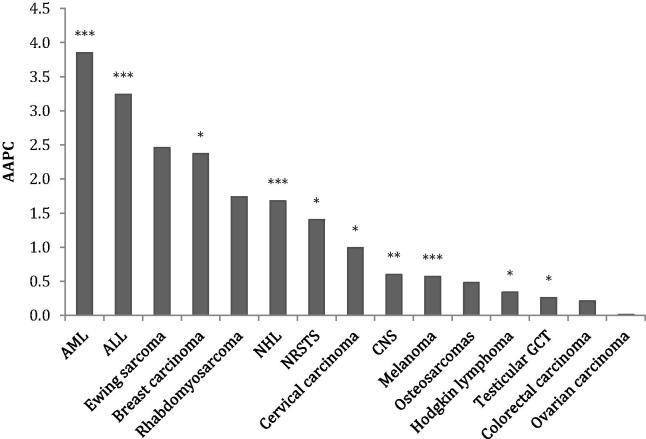
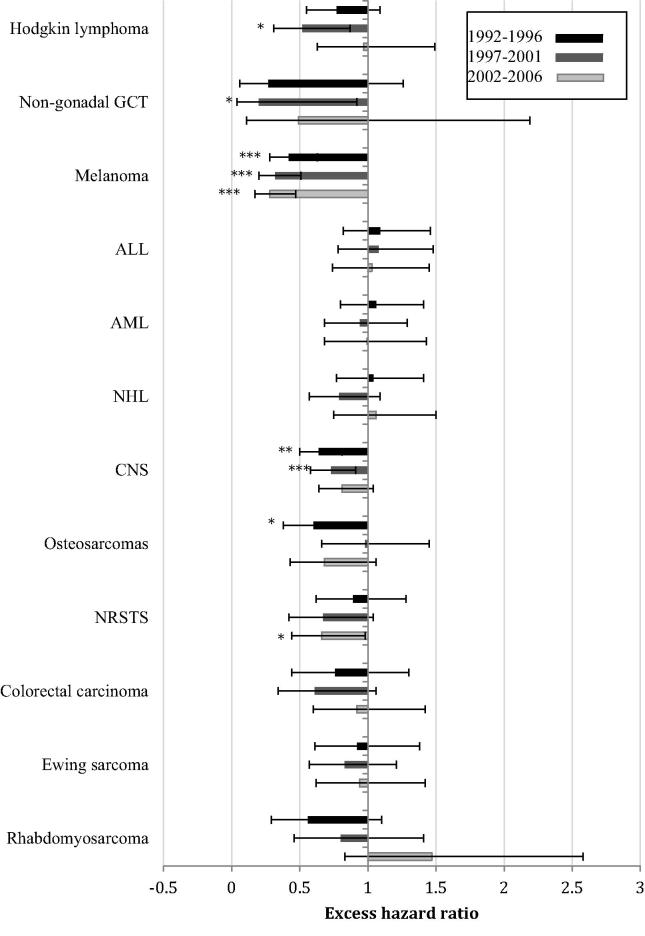
Results: Five-year survival for all cancers combined increased from 75.5% in 1992-1996 to 82.2% in 2002-2006 (P<0.001). Statistically significant improvements were seen for all disease groups except osteosarcoma, rhabdomyosarcoma, non-gonadal and ovarian germ cell tumours and ovarian and thyroid carcinomas. During the earliest time period, females had significantly better survival than males for five of the twelve non-gender-specific disease groups. By the latest period, only melanomas and non-rhabdomyosarcoma soft tissue sarcomas had differential survival by gender. Survival in the UK for the most recent period was generally similar to other comparable countries.
Conclusion: Five-year survival has improved considerably in the UK for most cancer types. For some disease groups, there has been little progress, either because survival already approaches 100% (e.g. thyroid carcinomas) or, more worryingly for some cancers with poor outcomes, because they remain resistant to existing therapy (e.g. rhabdomyosarcoma). In addition, for a number of specific cancer types and for cancer as a whole males continue to have worse outcomes than females.
Keywords: Adolescent; Cancer; Outcomes; Survival; TYA; Teenage; Trends; UK.
Copyright © 2015 The Authors. Published by Elsevier Ltd.. All rights reserved.
Figures
References
-
- Albritton K., Bleyer W.A. The management of cancer in the older adolescent. Eur J Cancer. 2003;39(18):2584–2599. - PubMed
-
- Fern L., Davies S., Eden T., Feltbower R., Grant R., Hawkins M. Rates of inclusion of teenagers and young adults in England into National Cancer Research Network clinical trials: report from the National Cancer Research Institute (NCRI) teenage and young adult clinical studies development group. Br J Cancer. 2008;99(12):1967–1974. - PMC - PubMed
-
- Whelan J.S., Fern L.A. Poor accrual of teenagers and young adults into clinical trials in the UK. Lancet Oncol. 2008;9(4):306–307. - PubMed
-
- Gatta G., Zigon G., Capocaccia R., Coebergh J.W., Desandes E., Kaatsch P. Survival of European children and young adults with cancer diagnosed 1995–2002. Eur J Cancer. 2009;45(6):992–1005. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
