

Comparative efficacy of interventions to promote hand hygiene in hospital: systematic review and network meta-analysis
- PMID: 26220070
- PMCID: PMC4517539
- DOI: 10.1136/bmj.h3728
Comparative efficacy of interventions to promote hand hygiene in hospital: systematic review and network meta-analysis
Abstract
Objective: To evaluate the relative efficacy of the World Health Organization 2005 campaign (WHO-5) and other interventions to promote hand hygiene among healthcare workers in hospital settings and to summarize associated information on use of resources.
Design: Systematic review and network meta-analysis.
Data sources: Medline, Embase, CINAHL, NHS Economic Evaluation Database, NHS Centre for Reviews and Dissemination, Cochrane Library, and the EPOC register (December 2009 to February 2014); studies selected by the same search terms in previous systematic reviews (1980-2009).
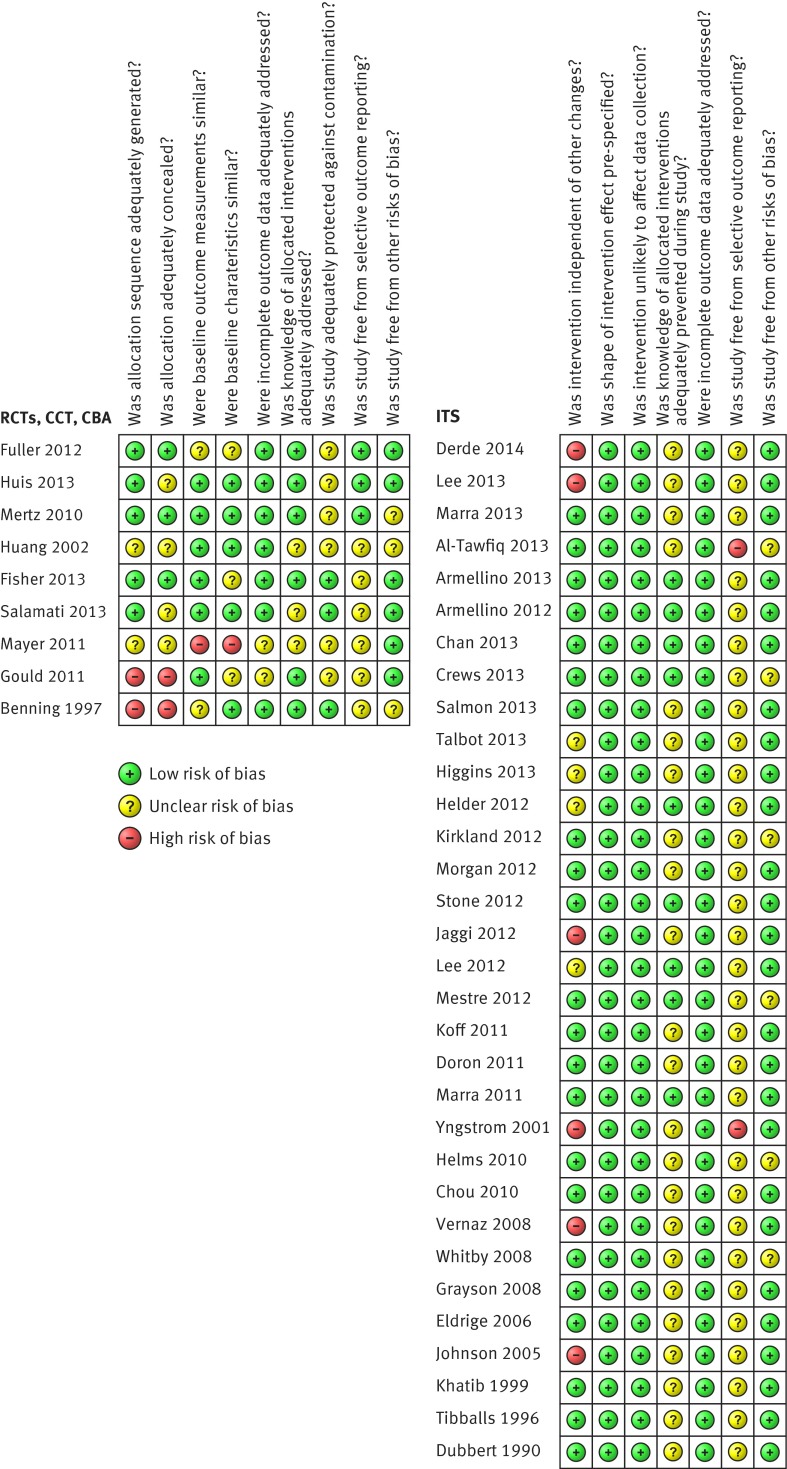
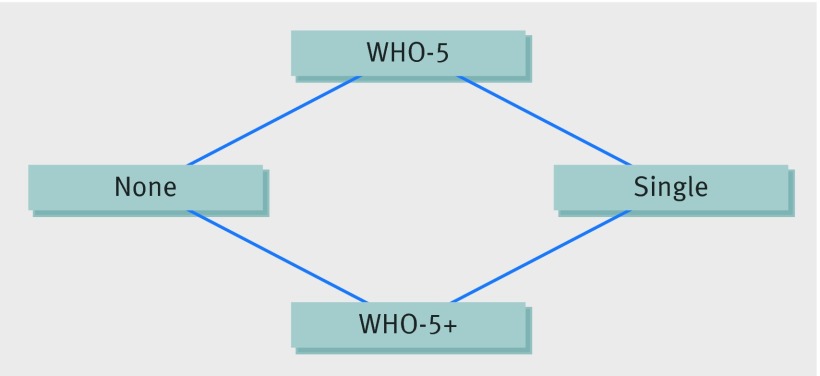
Review methods: Included studies were randomised controlled trials, non-randomised trials, controlled before-after trials, and interrupted time series studies implementing an intervention to improve compliance with hand hygiene among healthcare workers in hospital settings and measuring compliance or appropriate proxies that met predefined quality inclusion criteria. When studies had not used appropriate analytical methods, primary data were re-analysed. Random effects and network meta-analyses were performed on studies reporting directly observed compliance with hand hygiene when they were considered sufficiently homogeneous with regard to interventions and participants. Information on resources required for interventions was extracted and graded into three levels.
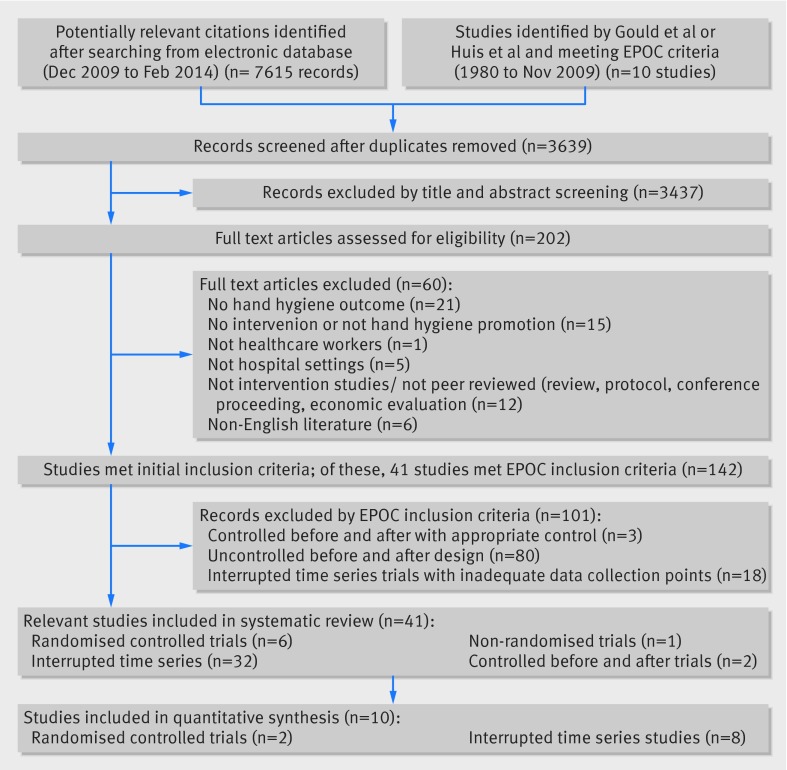
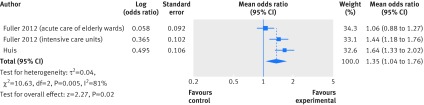
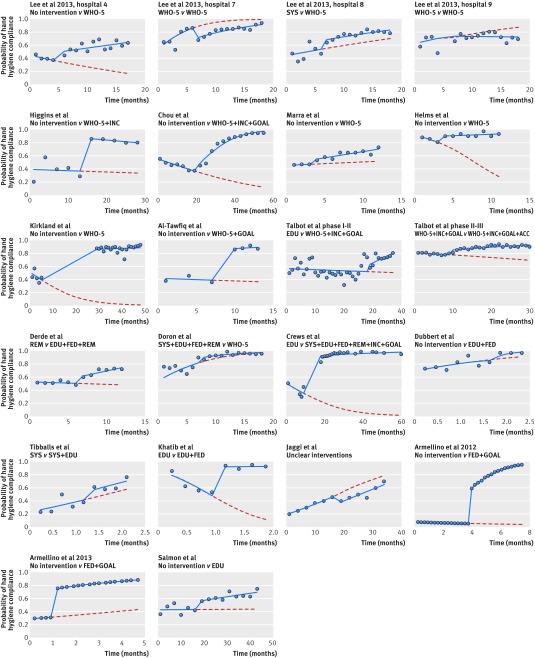
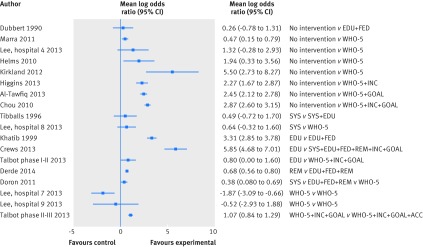
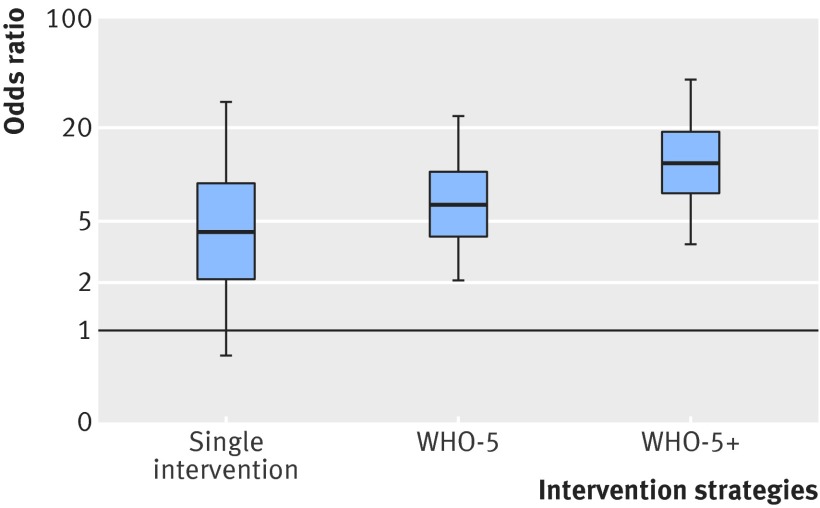
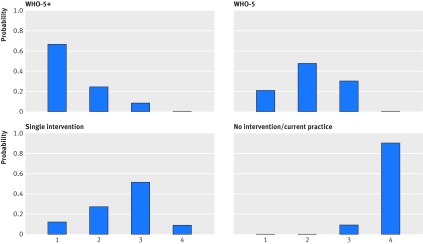
Results: Of 3639 studies retrieved, 41 met the inclusion criteria (six randomised controlled trials, 32 interrupted time series, one non-randomised trial, and two controlled before-after studies). Meta-analysis of two randomised controlled trials showed the addition of goal setting to WHO-5 was associated with improved compliance (pooled odds ratio 1.35, 95% confidence interval 1.04 to 1.76; I(2)=81%). Of 22 pairwise comparisons from interrupted time series, 18 showed stepwise increases in compliance with hand hygiene, and all but four showed a trend for increasing compliance after the intervention. Network meta-analysis indicated considerable uncertainty in the relative effectiveness of interventions, but nonetheless provided evidence that WHO-5 is effective and that compliance can be further improved by adding interventions including goal setting, reward incentives, and accountability. Nineteen studies reported clinical outcomes; data from these were consistent with clinically important reductions in rates of infection resulting from improved hand hygiene for some but not all important hospital pathogens. Reported costs of interventions ranged from $225 to $4669 (£146-£3035; €204-€4229) per 1000 bed days.
Conclusion: Promotion of hand hygiene with WHO-5 is effective at increasing compliance in healthcare workers. Addition of goal setting, reward incentives, and accountability strategies can lead to further improvements. Reporting of resources required for such interventions remains inadequate.
© Luangasanatip et al 2015.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Improving hand hygiene in hospitals--more is better.BMJ. 2015 Jul 28;351:h3931. doi: 10.1136/bmj.h3931. BMJ. 2015. PMID: 26220071 No abstract available.
-
Don't forget hand care when promoting hand hygiene in hospitals.BMJ. 2015 Aug 18;351:h4436. doi: 10.1136/bmj.h4436. BMJ. 2015. PMID: 26285710 No abstract available.
-
[WHO-5-campaign is successful].Dtsch Med Wochenschr. 2015 Oct;140(21):1572. doi: 10.1055/s-0041-104368. Epub 2015 Oct 21. Dtsch Med Wochenschr. 2015. PMID: 26488090 German. No abstract available.
References
-
- Jarvis WR. Selected aspects of the socioeconomic impact of nosocomial infections: morbidity, mortality, cost, and prevention. Infect Control Hosp Epidemiol 1996;17:552-7. - PubMed
-
- Rosenthal VD, Maki DG, Jamulitrat S, et al. International Nosocomial Infection Control Consortium (INICC) report, data summary for 2003-2008, issued June 2009. Am J Infect Control 2010;38:95-104.e2 - PubMed
-
- WHO guidelines on hand hygiene in health care (First global patient safety challenge clean care is safer care). WHO, 2009. - PubMed
-
- Gould DJ, Moralejo D, Drey N, Chudleigh JH, Interventions to improve hand hygiene compliance in patient care. Cochrane Database Syst Rev 2011:9:CD005186. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous