

Pediatric Cystic Fibrosis Sputum Can Be Chemically Dynamic, Anoxic, and Extremely Reduced Due to Hydrogen Sulfide Formation
- PMID: 26220964
- PMCID: PMC4551978
- DOI: 10.1128/mBio.00767-15
Pediatric Cystic Fibrosis Sputum Can Be Chemically Dynamic, Anoxic, and Extremely Reduced Due to Hydrogen Sulfide Formation
Abstract
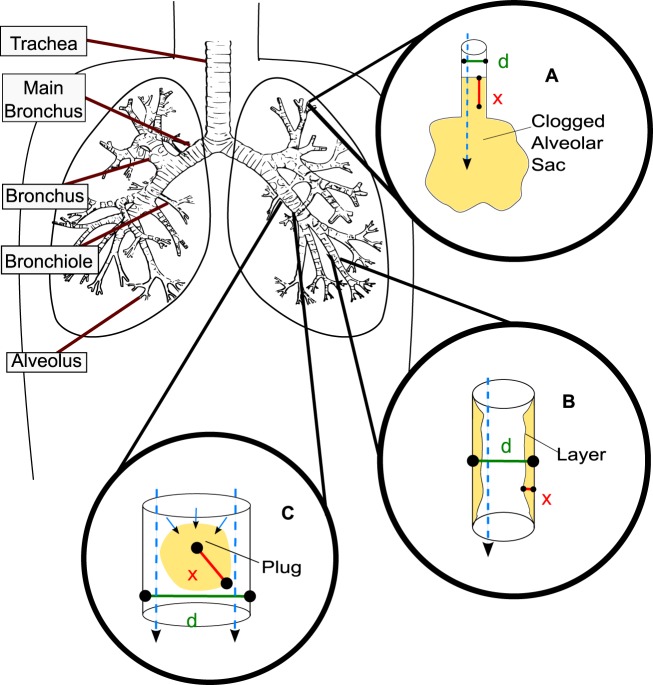
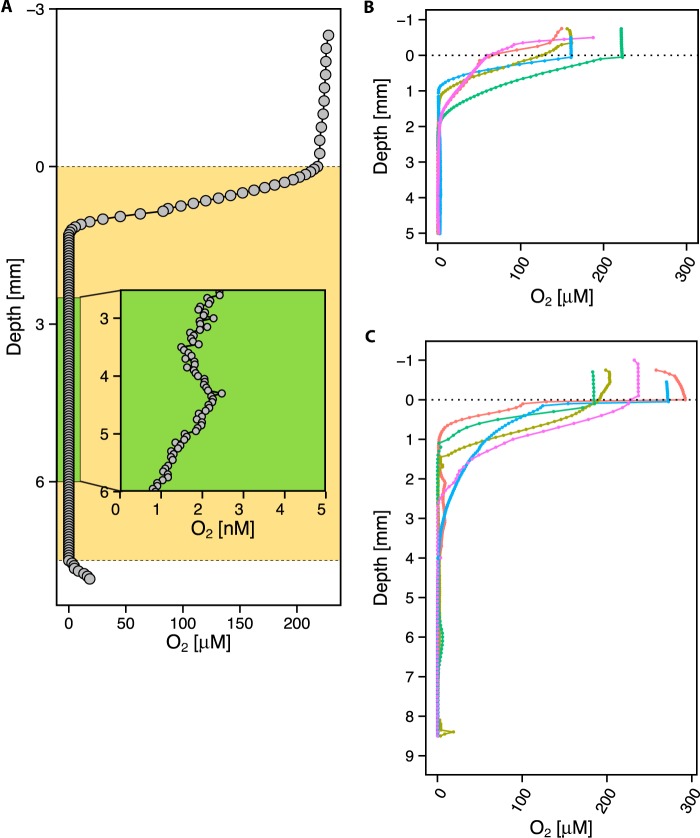
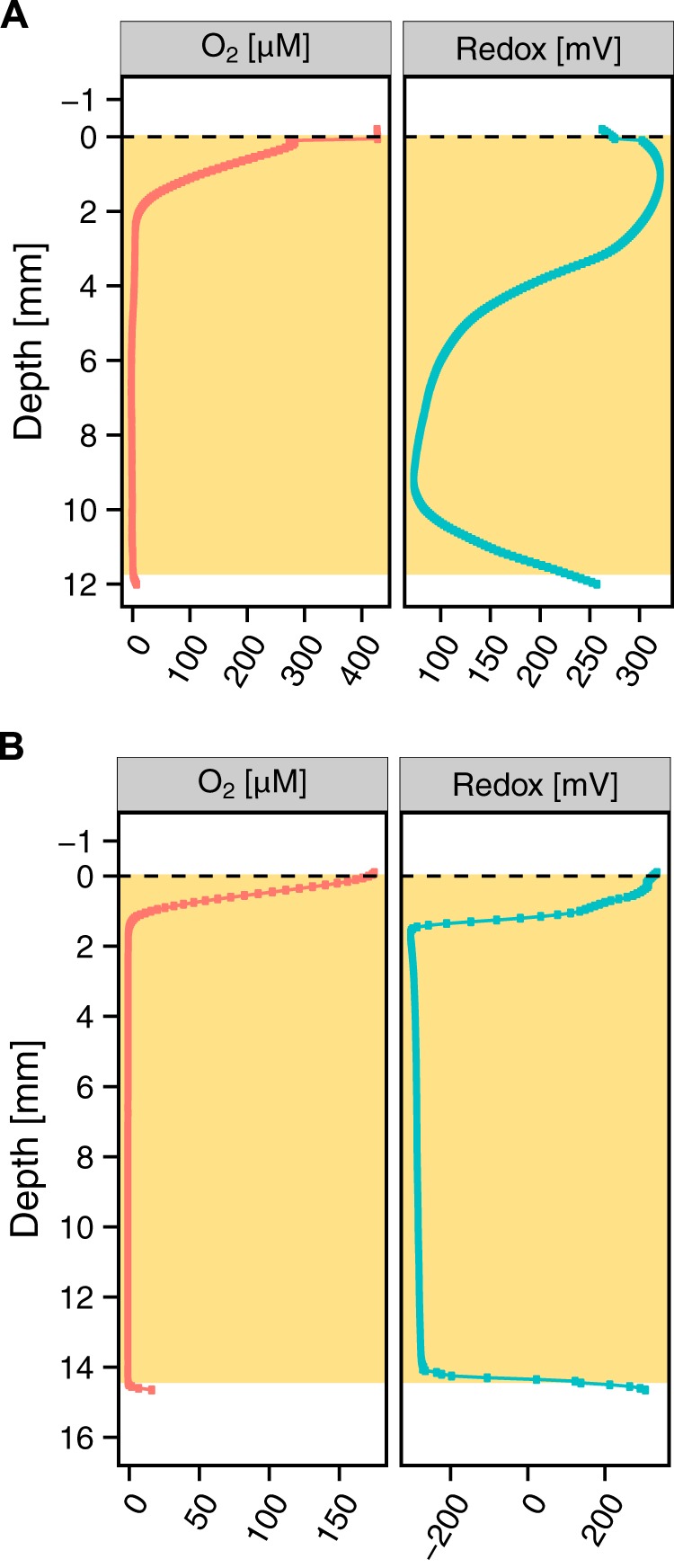
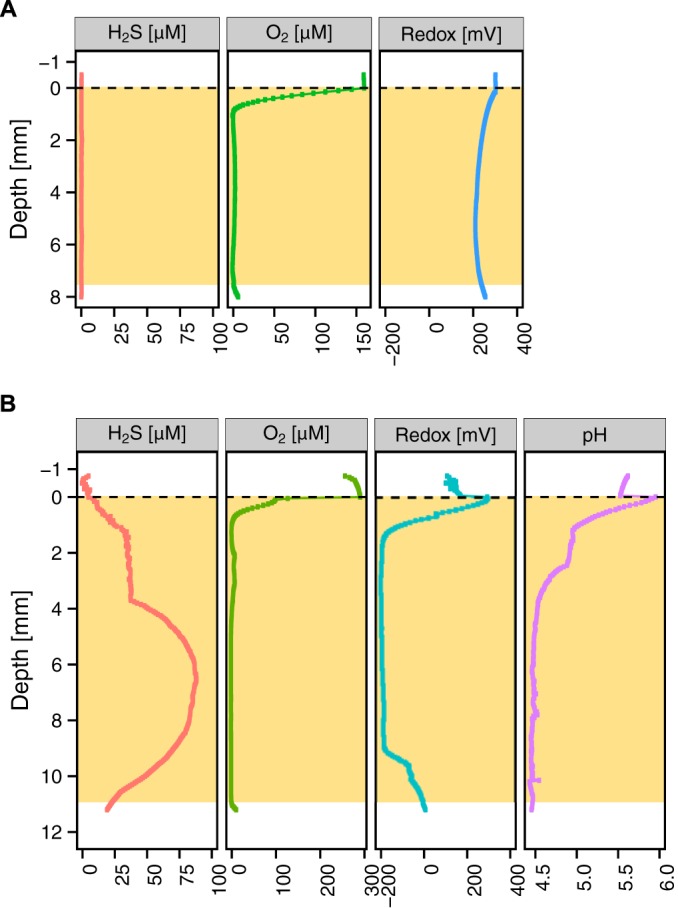
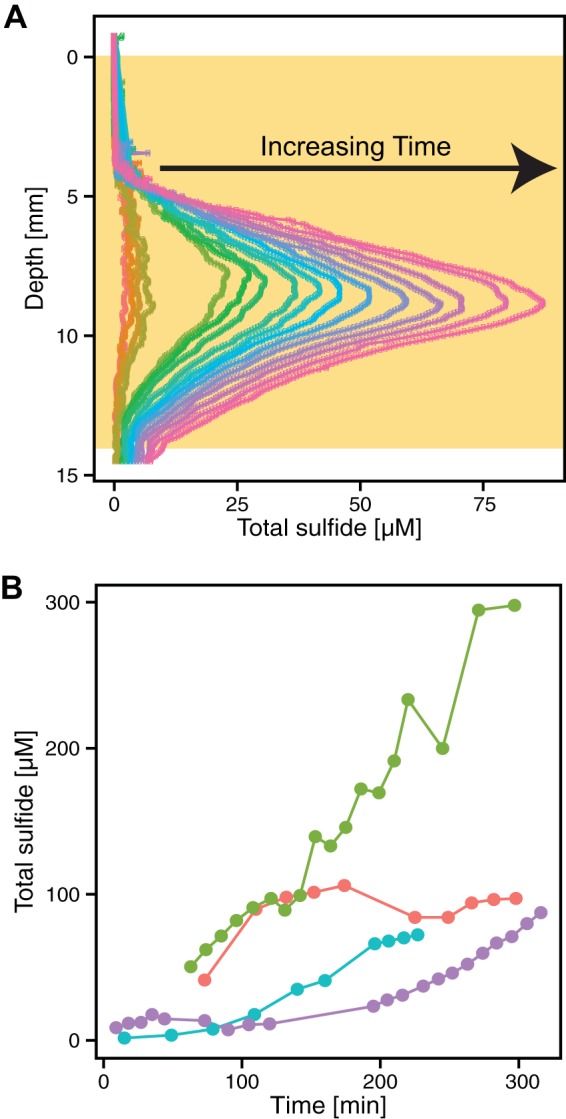
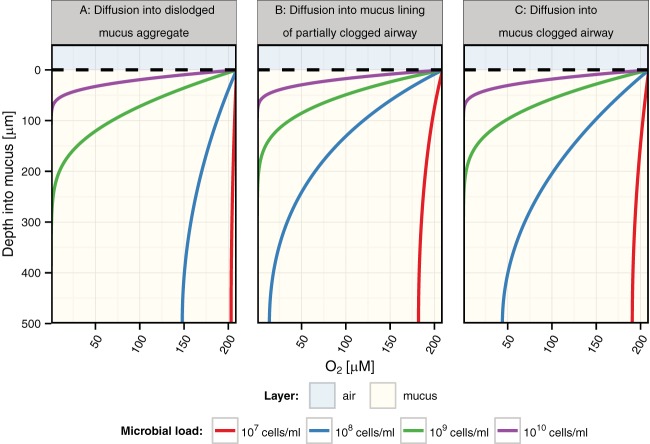
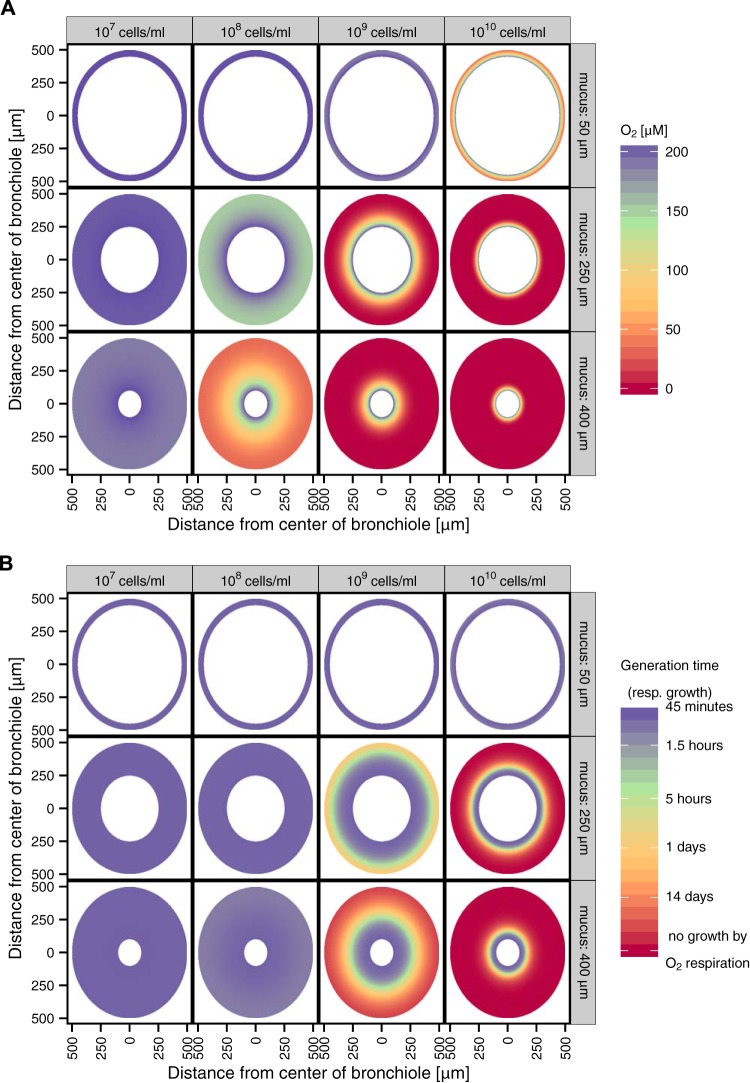
Severe and persistent bacterial lung infections characterize cystic fibrosis (CF). While several studies have documented the microbial diversity within CF lung mucus, we know much less about the inorganic chemistry that constrains microbial metabolic processes and their distribution. We hypothesized that sputum is chemically heterogeneous both within and between patients. To test this, we measured microprofiles of oxygen and sulfide concentrations as well as pH and oxidation-reduction potentials in 48 sputum samples from 22 pediatric patients with CF. Inorganic ions were measured in 20 samples from 12 patients. In all cases, oxygen was depleted within the first few millimeters below the sputum-air interface. Apart from this steep oxycline, anoxia dominated the sputum environment. Different sputum samples exhibited a broad range of redox conditions, with either oxidizing (16 mV to 355 mV) or reducing (-300 to -107 mV) potentials. The majority of reduced samples contained hydrogen sulfide and had a low pH (2.9 to 6.5). Sulfide concentrations increased at a rate of 0.30 µM H2S/min. Nitrous oxide was detected in only one sample that also contained sulfide. Microenvironmental variability was observed both within a single patient over time and between patients. Modeling oxygen dynamics within CF mucus plugs indicates that anoxic zones vary as a function of bacterial load and mucus thickness and can occupy a significant portion of the mucus volume. Thus, aerobic respiration accounts only partially for pathogen survival in CF sputum, motivating research to identify mechanisms of survival under conditions that span fluctuating redox states, including sulfidic environments.
Importance: Microbial infections are the major cause of morbidity and mortality in people living with CF, and yet microbial growth and survival in CF airways are not well understood. Insufficient information about the chemistry of the in vivo environment contributes to this knowledge gap. Our documentation of variable redox states corresponding to the presence or absence of sulfide begins to fill this void and motivates understanding of how different opportunistic pathogens adapt in these dynamic environments. Given the changing chemical state of CF sputum over time, it is important to consider a spectrum of aerobic and anaerobic lifestyles when studying CF pathogens in the laboratory. This work not only provides relevant constraints that can shape the design of laboratory experiments, it also suggests that sulfide might be a useful proxy for assessing the redox state of sputum in the clinic.
Copyright © 2015 Cowley et al.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
