

Efficacy and safety of luseogliflozin added to various oral antidiabetic drugs in Japanese patients with type 2 diabetes mellitus
- PMID: 26221523
- PMCID: PMC4511304
- DOI: 10.1111/jdi.12316
Efficacy and safety of luseogliflozin added to various oral antidiabetic drugs in Japanese patients with type 2 diabetes mellitus
Abstract
Introduction: Two studies were carried out to investigate the efficacy and safety of luseogliflozin added to existing oral antidiabetic drugs (OADs) in Japanese type 2 diabetic patients inadequately controlled with OAD monotherapy.
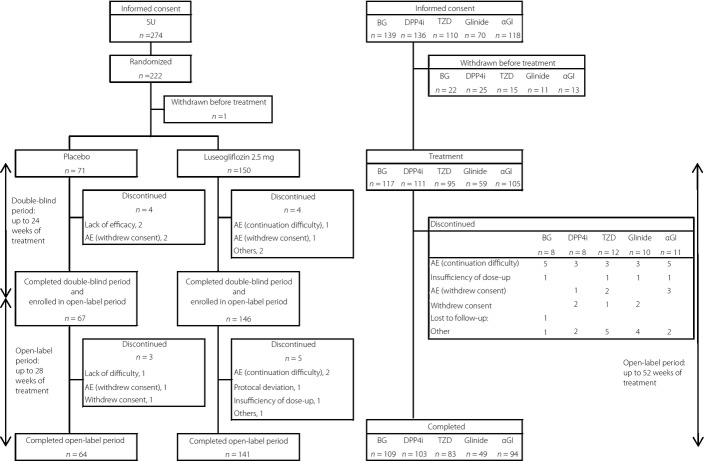
Materials and methods: In the trial involving add-on to sulfonylureas (study 03-1), patients were randomly assigned to receive luseogliflozin 2.5 mg or a placebo for a 24-week double-blind period, followed by a 28-week open-label period. In the open-label trial involving add-on to other OADs; that is, biguanides, dipeptidyl peptidase-4 inhibitors, thiazolidinediones, glinides and α-glucosidase inhibitors (study 03-2), patients received luseogliflozin for 52 weeks.
Results: In study 03-1, luseogliflozin significantly decreased glycated hemoglobin at the end of the 24-week double-blind period compared with the placebo (-0.88%, P < 0.001), and glycated hemoglobin reduction from baseline at week 52 was -0.63%. In study 03-2, luseogliflozin added to other OADs significantly decreased glycated hemoglobin from baseline at week 52 (-0.52 to -0.68%, P < 0.001 for all OADs). Bodyweight reduction was observed in all add-on therapies, even with agents associated with weight gain, such as sulfonylureas and thiazolidinediones. Most adverse events were mild in severity. When added to a sulfonylurea, incidences of hypoglycemia during the double-blind period were 8.7% and 4.2% for luseogliflozin and placebo, respectively, but no major hypoglycemic episodes occurred. The frequency and incidences of adverse events of special interest for sodium glucose cotransporter 2 inhibitors and adverse events associated with combined OADs were acceptable.
Conclusions: Add-on therapies of luseogliflozin to existing OADs improved glycemic control, reduced bodyweight and were well tolerated in Japanese type 2 diabetic patients. These trials were registered with the Japan Pharmaceutical Information Center (add on to sulfonylurea: JapicCTI-111507; add on to other OADs: JapicCTI-111508).
Keywords: Add-on therapy; Luseogliflozin; Oral antidiabetic drug.
Figures

References
-
- DeFronzo RA, Davidson JA, Del Prato S. The role of the kidneys in glucose homeostasis: a new path towards normalizing glycaemia. Diabetes Obes Metab. 2012;14:5–14. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
