

Pancreatectomy with vein reconstruction: technique matters
- PMID: 26223388
- PMCID: PMC4557658
- DOI: 10.1111/hpb.12463
Pancreatectomy with vein reconstruction: technique matters
Abstract
Background: A variety of techniques have been described for portal vein (PV) and/or superior mesenteric vein (SMV) resection/reconstruction during a pancreatectomy. The ideal strategy remains unclear.
Methods: Patients who underwent PV/SMV resection/reconstruction during a pancreatectomy from 2005 to 2014 were identified. Medical records and imaging were retrospectively reviewed for operative details and outcomes, with particular emphasis on patency.
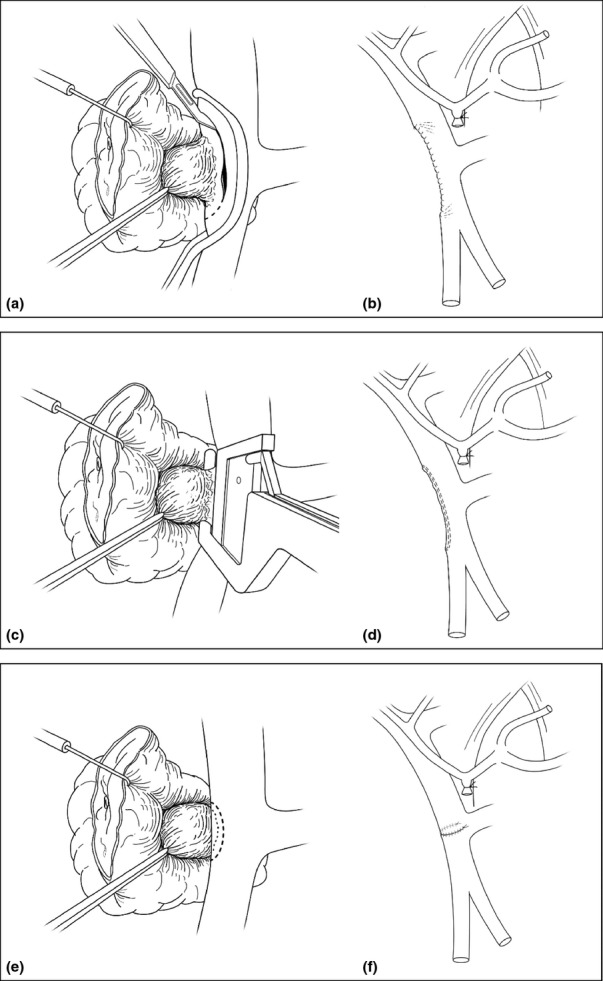
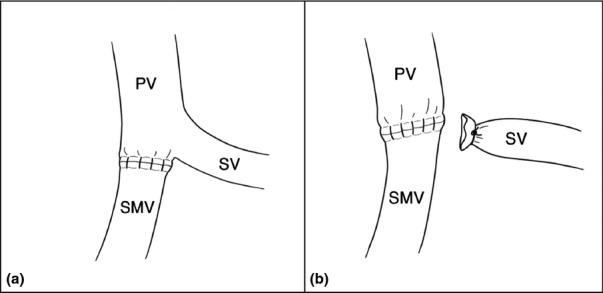
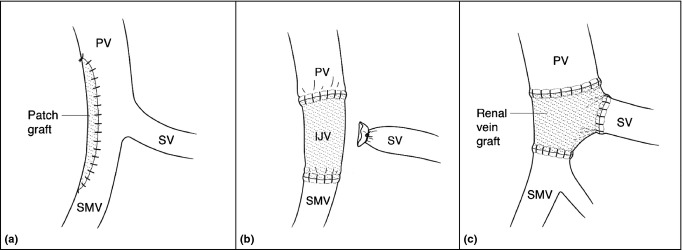
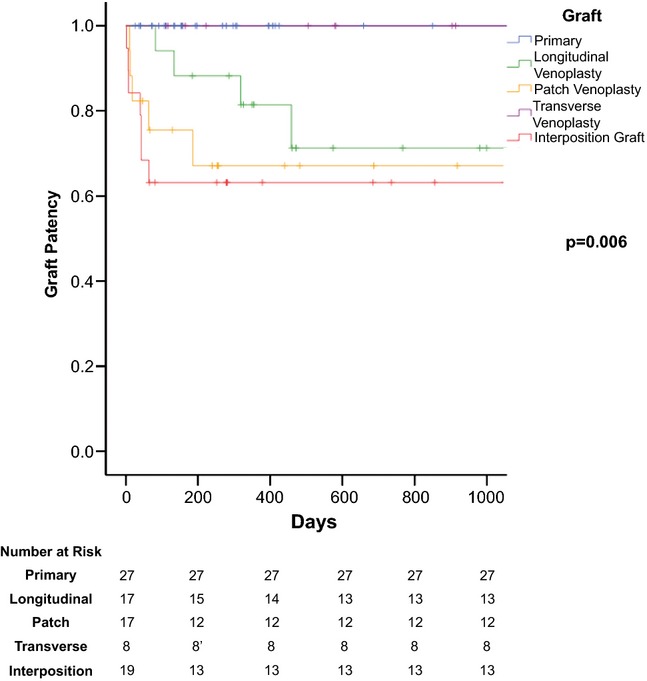
Results: Ninety patients underwent vein resection/reconstruction with one of five techniques: (i) longitudinal venorrhaphy (LV, n = 17); (ii) transverse venorrhaphy (TV, n = 9); (iii) primary end-to-end (n = 28); (iv) patch venoplasty (PV, n = 17); and (v) interposition graft (IG, n = 19). With a median follow-up of 316 days, thrombosis was observed in 16/90 (18%). The rate of thrombosis varied according to technique. All patients with primary end-to-end or TV remained patent. LV, PV and IG were all associated with significant rates of thrombosis (P = 0.001 versus no thrombosis). Comparing thrombosed to patent, there were no differences with respect to pancreatectomy type, pre-operative knowledge of vein involvement and neoadjuvant therapy. Prophylactic aspirin was used in 69% of the total cohort (66% of patent, 81% of thrombosed) and showed no protective benefit.
Conclusions: Primary end-to-end and TV have superior patency than the alternatives after PV/SMV resection and should be the preferred techniques for short (<3 cm) reconstructions.
© 2015 International Hepato-Pancreato-Biliary Association.
Figures
References
-
- Tseng JF, Raut CP, Lee JE, Pisters PW, Vauthey JN, Abdalla EK, et al. Pancreaticoduodenectomy with vascular resection: margin status and survival duration. J Gastrointest Surg. 2004;8:935–949. discussion 49–50. - PubMed
-
- Toomey P, Hernandez J, Morton C, Duce L, Farrior T, Villadolid D, et al. Resection of portovenous structures to obtain microscopically negative margins during pancreaticoduodenectomy for pancreatic adenocarcinoma is worthwhile. Am Surg. 2009;75:804–809. discussion 9–10. - PubMed
-
- Evans DB, Farnell MB, Lillemoe KD, Vollmer C, Jr, Strasberg SM, Schulick RD. Surgical treatment of resectable and borderline resectable pancreas cancer: expert consensus statement. Ann Surg Oncol. 2009;16:1736–1744. - PubMed
-
- Haugvik SP, Labori KJ, Waage A, Line PD, Mathisen O, Gladhaug IP. Pancreatic surgery with vascular reconstruction in patients with locally advanced pancreatic neuroendocrine tumors. J Gastrointest Surg. 2013;17:1224–1232. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
