

The UK-PBC risk scores: Derivation and validation of a scoring system for long-term prediction of end-stage liver disease in primary biliary cholangitis
- PMID: 26223498
- PMCID: PMC6984963
- DOI: 10.1002/hep.28017
The UK-PBC risk scores: Derivation and validation of a scoring system for long-term prediction of end-stage liver disease in primary biliary cholangitis
Abstract
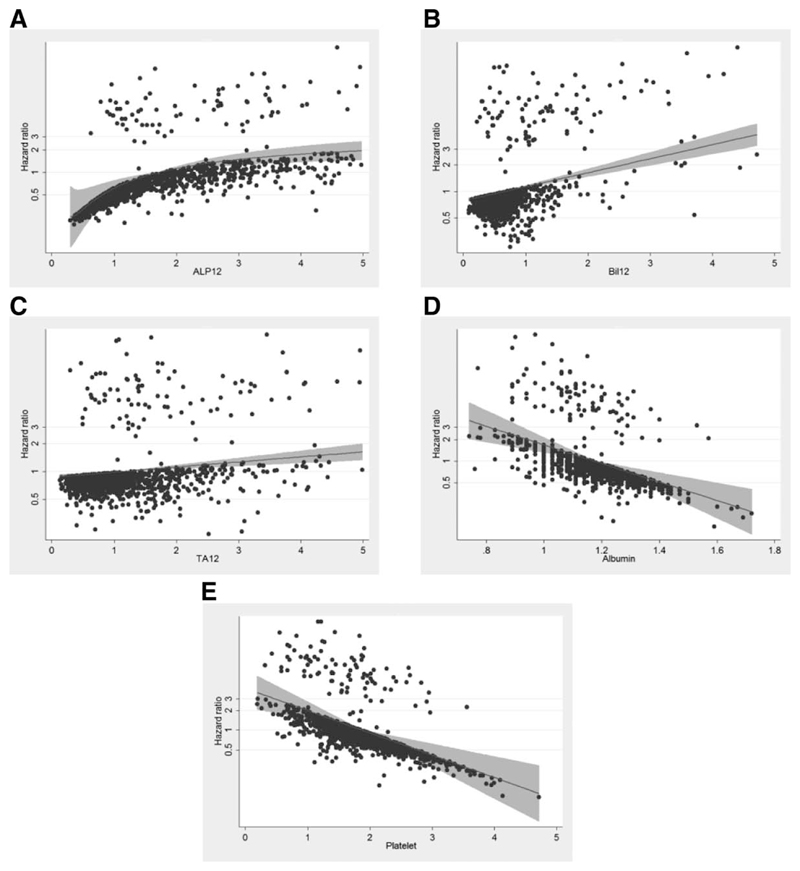
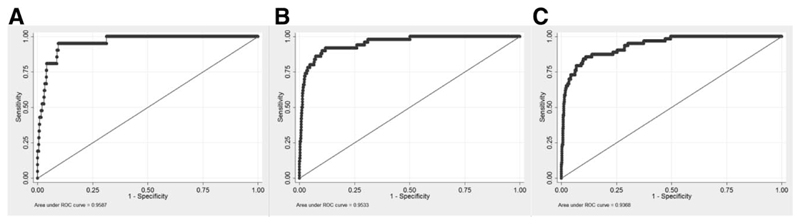
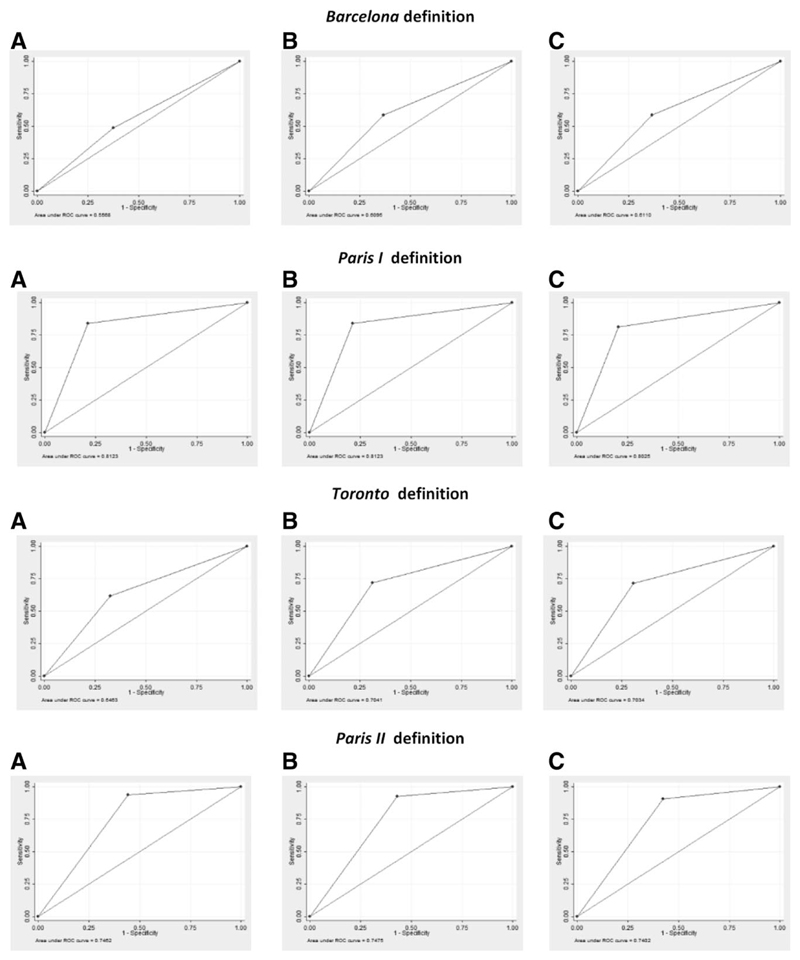
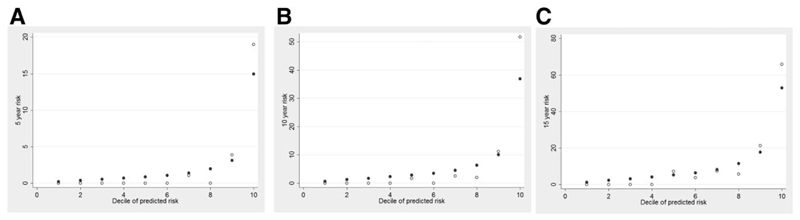
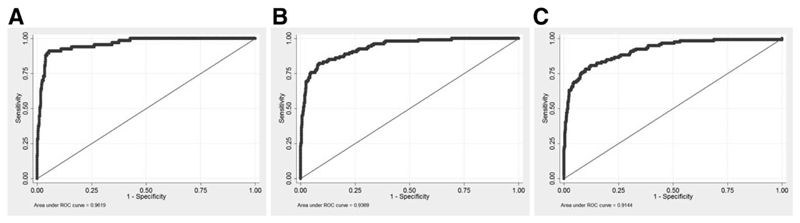
The biochemical response to ursodeoxycholic acid (UDCA)--so-called "treatment response"--strongly predicts long-term outcome in primary biliary cholangitis (PBC). Several long-term prognostic models based solely on the treatment response have been developed that are widely used to risk stratify PBC patients and guide their management. However, they do not take other prognostic variables into account, such as the stage of the liver disease. We sought to improve existing long-term prognostic models of PBC using data from the UK-PBC Research Cohort. We performed Cox's proportional hazards regression analysis of diverse explanatory variables in a derivation cohort of 1,916 UDCA-treated participants. We used nonautomatic backward selection to derive the best-fitting Cox model, from which we derived a multivariable fractional polynomial model. We combined linear predictors and baseline survivor functions in equations to score the risk of a liver transplant or liver-related death occurring within 5, 10, or 15 years. We validated these risk scores in an independent cohort of 1,249 UDCA-treated participants. The best-fitting model consisted of the baseline albumin and platelet count, as well as the bilirubin, transaminases, and alkaline phosphatase, after 12 months of UDCA. In the validation cohort, the 5-, 10-, and 15-year risk scores were highly accurate (areas under the curve: >0.90).
Conclusions: The prognosis of PBC patients can be accurately evaluated using the UK-PBC risk scores. They may be used to identify high-risk patients for closer monitoring and second-line therapies, as well as low-risk patients who could potentially be followed up in primary care.
© 2015 by the American Association for the Study of Liver Diseases.
Conflict of interest statement
Potential conflict of interest: Dr. Hirschfield advises Intercept and is on the speakers’ bureau for Falk. Dr. Williamson consults for Intercept. Dr. Sandford consults for Otsuka and received grants from Intercept. Dr. Heneghan received grants from Astellas.
Figures
Comment in
-
Predicting risk in primary biliary cholangitis.Hepatology. 2016 Mar;63(3):697-9. doi: 10.1002/hep.28377. Epub 2016 Jan 14. Hepatology. 2016. PMID: 26638198 No abstract available.
References
-
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: management of cholestatic liver diseases. J Hepatol. 2009;51:237–267. - PubMed
-
- Carbone M, Mells GF, Pells G, Dawwas MF, Newton JL, Heneghan MA, et al. Sex and age are determinants of the clinical phenotype of primary biliary cirrhosis and response to ursodeoxycholic acid. Gastroenterology. 2013;144:560–569.e7. quiz, e513-e564. - PubMed
-
- Poupon RE, Poupon R, Balkau B. Ursodiol for the long-term treatment of primary biliary cirrhosis. The UDCA-PBC Study Group. N Engl J Med. 1994;330:1342–1347. - PubMed
-
- Lindor KD, Gershwin ME, Poupon R, Kaplan M, Bergasa NV, Heathcote EJ, American Association for Study of Liver Diseases Primary biliary cirrhosis. Hepatology. 2009;50:291–308. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
