

Optimal composite scores for longitudinal clinical trials under the linear mixed effects model
- PMID: 26223663
- PMCID: PMC5132034
- DOI: 10.1002/pst.1701
Optimal composite scores for longitudinal clinical trials under the linear mixed effects model
Abstract
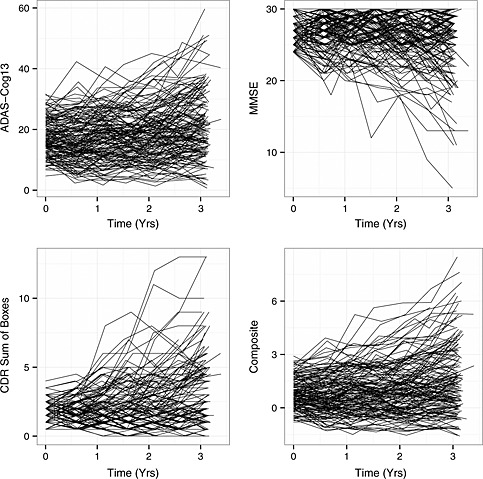
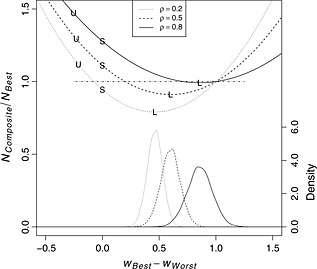
Clinical trials of chronic, progressive conditions use rate of change on continuous measures as the primary outcome measure, with slowing of progression on the measure as evidence of clinical efficacy. For clinical trials with a single prespecified primary endpoint, it is important to choose an endpoint with the best signal-to-noise properties to optimize statistical power to detect a treatment effect. Composite endpoints composed of a linear weighted average of candidate outcome measures have also been proposed. Composites constructed as simple sums or averages of component tests, as well as composites constructed using weights derived from more sophisticated approaches, can be suboptimal, in some cases performing worse than individual outcome measures. We extend recent research on the construction of efficient linearly weighted composites by establishing the often overlooked connection between trial design and composite performance under linear mixed effects model assumptions and derive a formula for calculating composites that are optimal for longitudinal clinical trials of known, arbitrary design. Using data from a completed trial, we provide example calculations showing that the optimally weighted linear combination of scales can improve the efficiency of trials by almost 20% compared with the most efficient of the individual component scales. Additional simulations and analytical results demonstrate the potential losses in efficiency that can result from alternative published approaches to composite construction and explore the impact of weight estimation on composite performance.
Keywords: Alzheimer's disease; composite; linear mixed effects model; longitudinal clinical trial; mild cognitive impairment.
Copyright © 2015 John Wiley & Sons, Ltd.
Figures
References
-
- Ard MC, Galasko DR, Edland SD. Improved statistical power of Alzheimer clinical trials by item response theory: proof of concept by application to the Activities of Daily Living Scale. Alzheimer Disease and Associated Disorders. 2013; 27(2):187–191. PMID: 22874658. doi: 10.1097/WAD.0b013e318265bcc1. - PMC - PubMed
-
- US Dept of Health and Human Services; US Food and Drug Administration; Center for Drug Evaluation and Research. Guidance for industry: Alzheimer's disease: developing drugs for the treatment of early stage disease (draft guidance). Available at: http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformati.... (Published February 2013. Accessed 19 June, 2014).
-
- Kozauer N, Katz R. Regulatory innovation and drug development for early‐stage Alzheimer's disease. The New England Journal of Medicine. 2013; 368(13):1169–1171. - PubMed
-
- Raghavan N, Samtani MN, Farnum M, Yang E, Novak G, Grundman M, Narayan V, DiBernardo A. The ADAS‐Cog revisited: novel composite scales based on ADAS‐Cog to improve efficiency in MCI and early AD trials. Alzheimers Dement. 2013; 9:S21–31, doi:10.1016/j.jalz.2012.05.2187. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
