

Response to endovascular reperfusion is not time-dependent in patients with salvageable tissue
- PMID: 26224727
- PMCID: PMC4553034
- DOI: 10.1212/WNL.0000000000001853
Response to endovascular reperfusion is not time-dependent in patients with salvageable tissue
Abstract
Objective: To evaluate whether time to treatment modifies the effect of endovascular reperfusion in stroke patients with evidence of salvageable tissue on MRI.
Methods: Patients from the Diffusion and Perfusion Imaging Evaluation for Understanding Stroke Evolution 2 (DEFUSE 2) cohort study with a perfusion-diffusion target mismatch were included. Reperfusion was defined as a decrease in the perfusion lesion volume of at least 50% between baseline and early follow-up. Good functional outcome was defined as a modified Rankin Scale score ≤2 at day 90. Lesion growth was defined as the difference between the baseline and the early follow-up diffusion-weighted imaging lesion volumes.
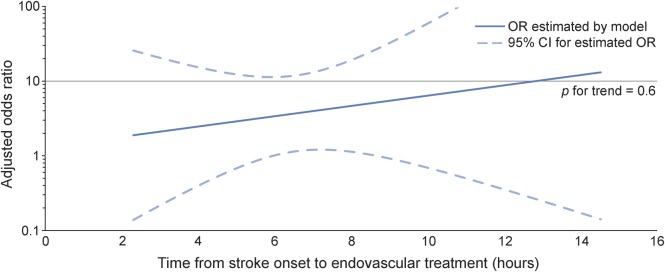
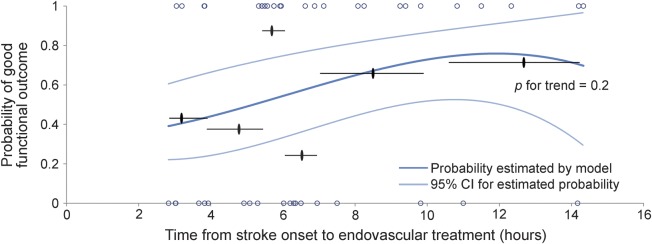
Results: Among 78 patients with the target mismatch profile (mean age 66 ± 16 years, 54% women), reperfusion was associated with increased odds of good functional outcome (adjusted odds ratio 3.7, 95% confidence interval 1.2-12, p = 0.03) and attenuation of lesion growth (p = 0.02). Time to treatment did not modify these effects (p value for the time × reperfusion interaction is 0.6 for good functional outcome and 0.3 for lesion growth). Similarly, in the subgroup of patients with reperfusion (n = 46), time to treatment was not associated with good functional outcome (p = 0.2).
Conclusion: The association between endovascular reperfusion and improved functional and radiologic outcomes is not time-dependent in patients with a perfusion-diffusion mismatch. Proof that patients with mismatch benefit from endovascular therapy in the late time window should come from a randomized placebo-controlled trial.
© 2015 American Academy of Neurology.
Figures

References
-
- Campbell BCV, Mitchell PJ, Kleinig TJ, et al. ; EXTEND-IA Investigators. Endovascular therapy for ischemic stroke with perfusion-imaging selection. N Engl J Med 2015;372:1009–1018. - PubMed
-
- Goyal M, Demchuk AM, Menon BK, et al. ; ESCAPE Trial Investigators. Randomized assessment of rapid endovascular treatment of ischemic stroke. N Engl J Med 2015;372:1019–1030. - PubMed
-
- Berkhemer OA, Fransen PSS, Beumer D, et al. ; MR CLEAN Investigators. A randomized trial of intraarterial treatment for acute ischemic stroke. N Engl J Med 2015;372:11–20. - PubMed
-
- Saver J. Solitaire FR with the intention for thrombectomy as primary endovascular treatment for acute ischemic stroke: preliminary results. Presented at the International Stroke Conference; February 11, 2015; Nashville, TN. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical