

Clinical Risk Stratification for Primary Prevention Implantable Cardioverter Defibrillators
- PMID: 26224792
- PMCID: PMC4568903
- DOI: 10.1161/CIRCHEARTFAILURE.115.002414
Clinical Risk Stratification for Primary Prevention Implantable Cardioverter Defibrillators
Abstract
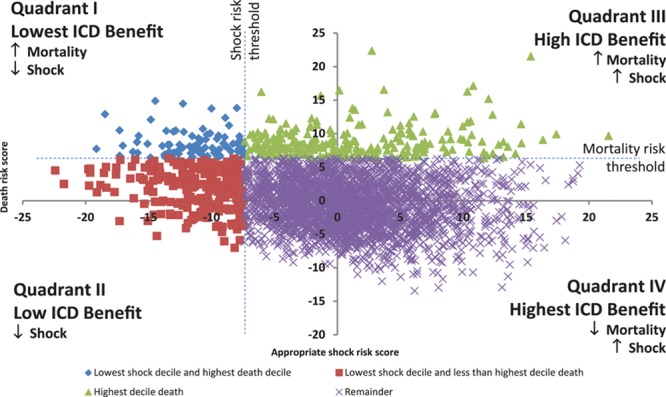
Background: A conceptualized model may be useful for understanding risk stratification of primary prevention implantable cardioverter defibrillators considering the competing risks of appropriate implantable cardioverter defibrillator shock versus mortality.
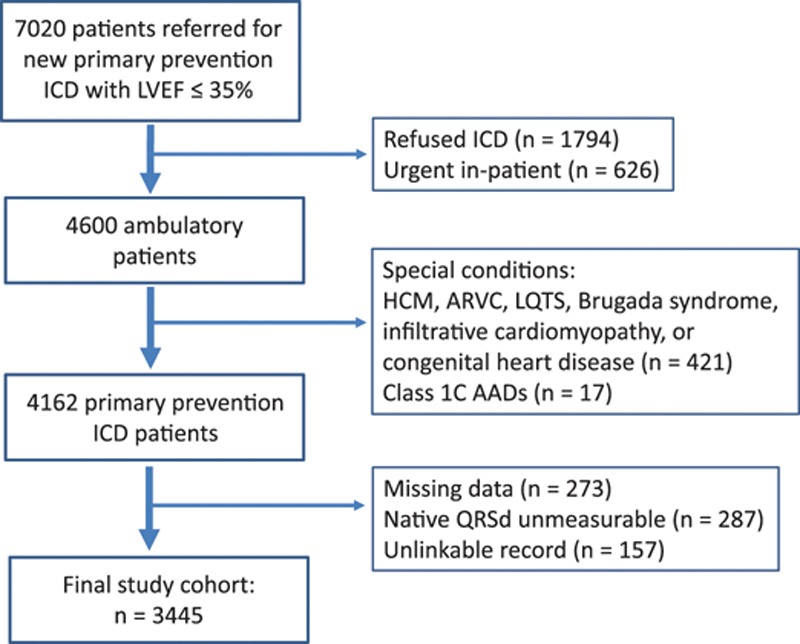
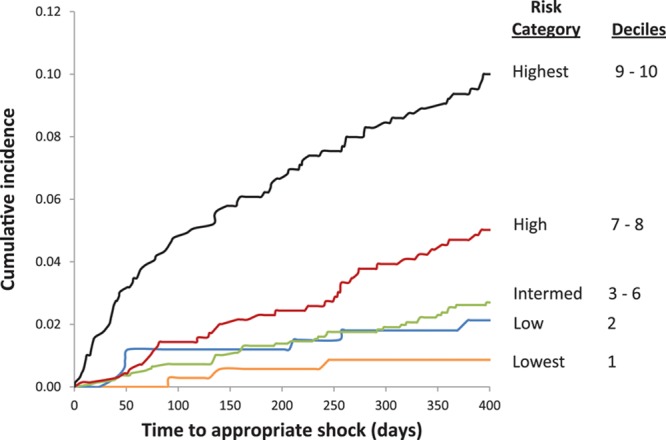
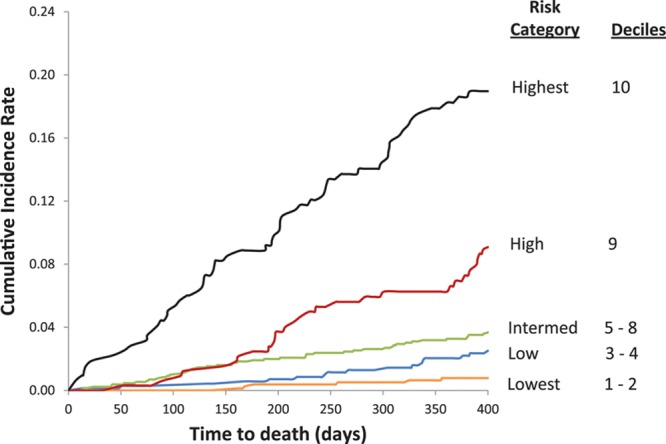
Methods and results: In a prospective, multicenter, population-based cohort with left ventricular ejection fraction ≤35% referred for primary prevention implantable cardioverter defibrillator, we developed dual risk stratification models to determine the competing risks of appropriate defibrillator shock versus mortality using a Fine-Gray subdistribution hazard model. Among 7020 patients referred, 3445 underwent defibrillator implant (79.7% men, median, 66 years [25th, 75th: 58-73]). During 5918 person-years of follow-up, appropriate shock occurred in 204 patients (3.6 shocks/100 person-years) and 292 died (4.9 deaths/100 person-years). Competing risk predictors of appropriate shock included nonsustained ventricular tachycardia, atrial fibrillation, serum creatinine concentration, digoxin or amiodarone use, and QRS duration near 130-ms peak. One-year cumulative incidence of appropriate shock was 0.9% in the lowest risk category, and 1.7%, 2.5%, 4.9%, and 9.3% in low, intermediate, high, and highest risk groups, respectively. Hazard ratios for appropriate shock ranged from 4.04 to 7.79 in the highest 3 deciles (all P≤0.001 versus lowest risk). Cumulative incidence of 1-year death was 0.6%, 1.9%, 3.3%, 6.2%, and 17.7% in lowest, low, intermediate, high, and highest risk groups, respectively. Mortality hazard ratios ranged from 11.48 to 36.22 in the highest 3 deciles (all P<0.001 versus lowest risk).
Conclusions: Simultaneous estimation of risks of appropriate shock and mortality can be performed using clinical variables, providing a potential framework for identification of patients who are unlikely to benefit from prophylactic implantable cardioverter defibrillator.
Keywords: cardiac arrhythmia; death; decision making; decision support techniques; sudden cardiac death; ventricular fibrillation; ventricular tachycardia.
© 2015 The Authors.
Figures
Comment in
-
Mapping the Terrain of Competing Risk Following Primary Prevention Defibrillator Implantation.Circ Heart Fail. 2015 Sep;8(5):847-9. doi: 10.1161/CIRCHEARTFAILURE.115.002503. Circ Heart Fail. 2015. PMID: 26374916 No abstract available.
References
-
- Bardy GH, Lee KL, Mark DB, Poole JE, Packer DL, Boineau R, Domanski M, Troutman C, Anderson J, Johnson G, McNulty SE, Clapp-Channing N, Davidson-Ray LD, Fraulo ES, Fishbein DP, Luceri RM, Ip JH Sudden Cardiac Death in Heart Failure Trial (SCD-HeFT) Investigators. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. N Engl J Med. 2005;352:225–237. doi: 10.1056/NEJMoa043399. - PubMed
-
- Moss AJ, Zareba W, Hall WJ, Klein H, Wilber DJ, Cannom DS, Daubert JP, Higgins SL, Brown MW, Andrews ML Multicenter Automatic Defibrillator Implantation Trial II Investigators. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med. 2002;346:877–883. doi: 10.1056/NEJMoa013474. - PubMed
-
- Lee DS, Gona P, Albano I, Larson MG, Benjamin EJ, Levy D, Kannel WB, Vasan RS. A systematic assessment of causes of death after heart failure onset in the community: impact of age at death, time period, and left ventricular systolic dysfunction. Circ Heart Fail. 2011;4:36–43. doi: 10.1161/CIRCHEARTFAILURE.110.957480. - PMC - PubMed
-
- Priori SG, Aliot E, Blomstrom-Lundqvist C, Bossaert L, Breithardt G, Brugada P, Camm AJ, Cappato R, Cobbe SM, Di Mario C, Maron BJ, McKenna WJ, Pedersen AK, Ravens U, Schwartz PJ, Trusz-Gluza M, Vardas P, Wellens HJ, Zipes DP. Task force on sudden cardiac death of the European Society of Cardiology. Eur Heart J. 2001;22:1374–1450. doi: 10.1053/euhj.2001.2824. - PubMed
-
- Fishman GI, Chugh SS, Dimarco JP, Albert CM, Anderson ME, Bonow RO, Buxton AE, Chen PS, Estes M, Jouven X, Kwong R, Lathrop DA, Mascette AM, Nerbonne JM, O’Rourke B, Page RL, Roden DM, Rosenbaum DS, Sotoodehnia N, Trayanova NA, Zheng ZJ. Sudden cardiac death prediction and prevention: report from a National Heart, Lung, and Blood Institute and Heart Rhythm Society Workshop. Circulation. 2010;122:2335–2348. doi: 10.1161/CIRCULATIONAHA.110.976092. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
