

Early versus delayed umbilical cord clamping in infants with congenital heart disease: a pilot, randomized, controlled trial
- PMID: 26226244
- PMCID: PMC5095614
- DOI: 10.1038/jp.2015.89
Early versus delayed umbilical cord clamping in infants with congenital heart disease: a pilot, randomized, controlled trial
Abstract
Objective: Delayed umbilical cord clamping (DCC) at birth may provide a better neonatal health status than early umbilical cord clamping (ECC). However, the safety and feasibility of DCC in infants with congenital heart disease (CHD) have not been tested. This was a pilot, randomized, controlled trial to establish the safety and feasibility of DCC in neonates with CHD.
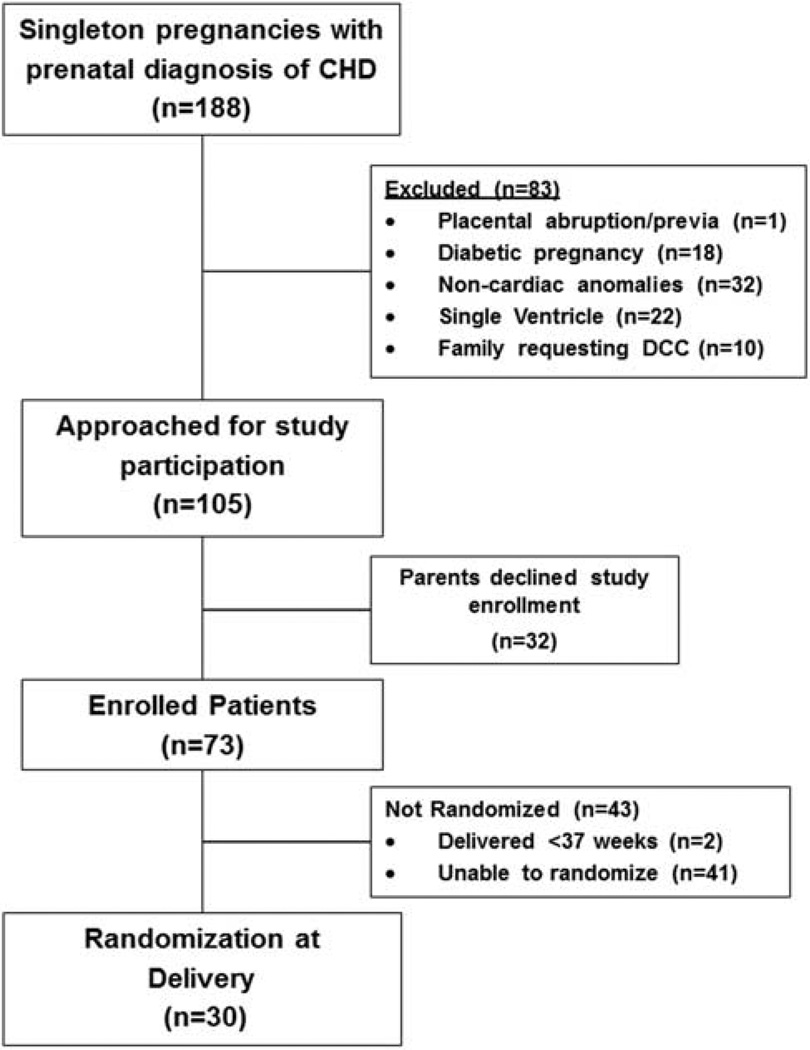
Study design: Pregnant women admitted >37 weeks gestational age with prenatal diagnosis of critical CHD were enrolled and randomized to ECC or DCC. For ECC, the umbilical cord was clamped <10 s after birth; for DCC, the cord was clamped ~120 s after delivery.
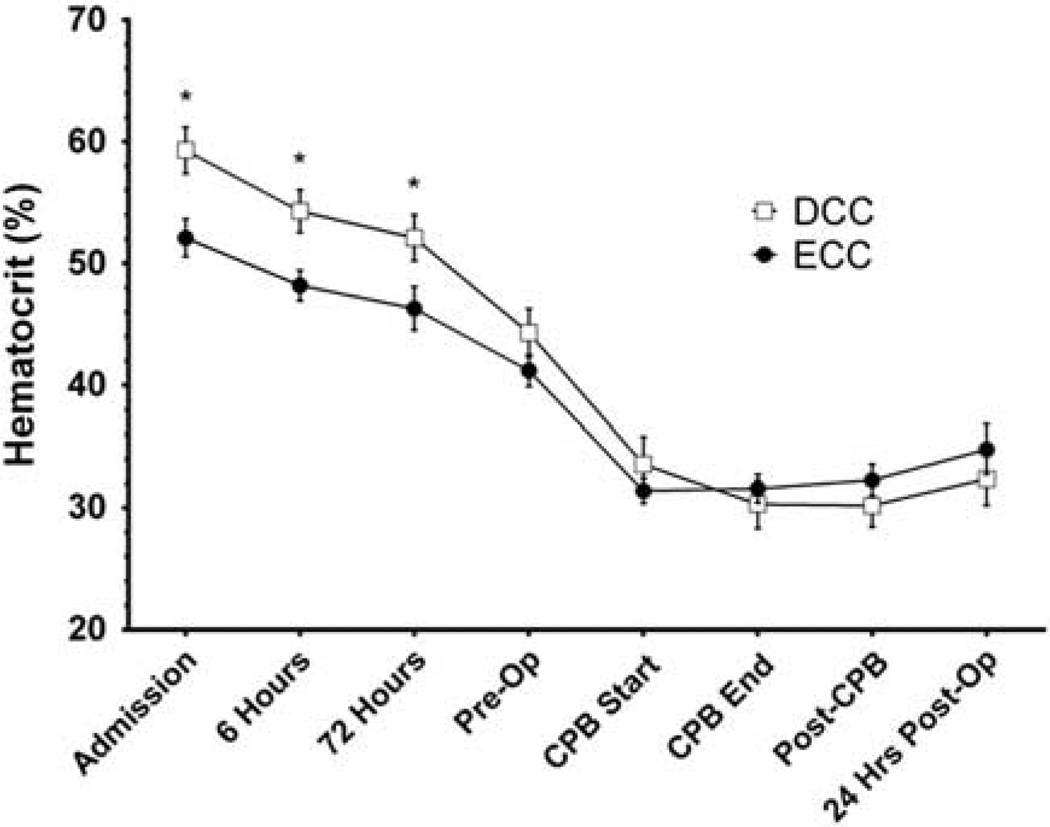
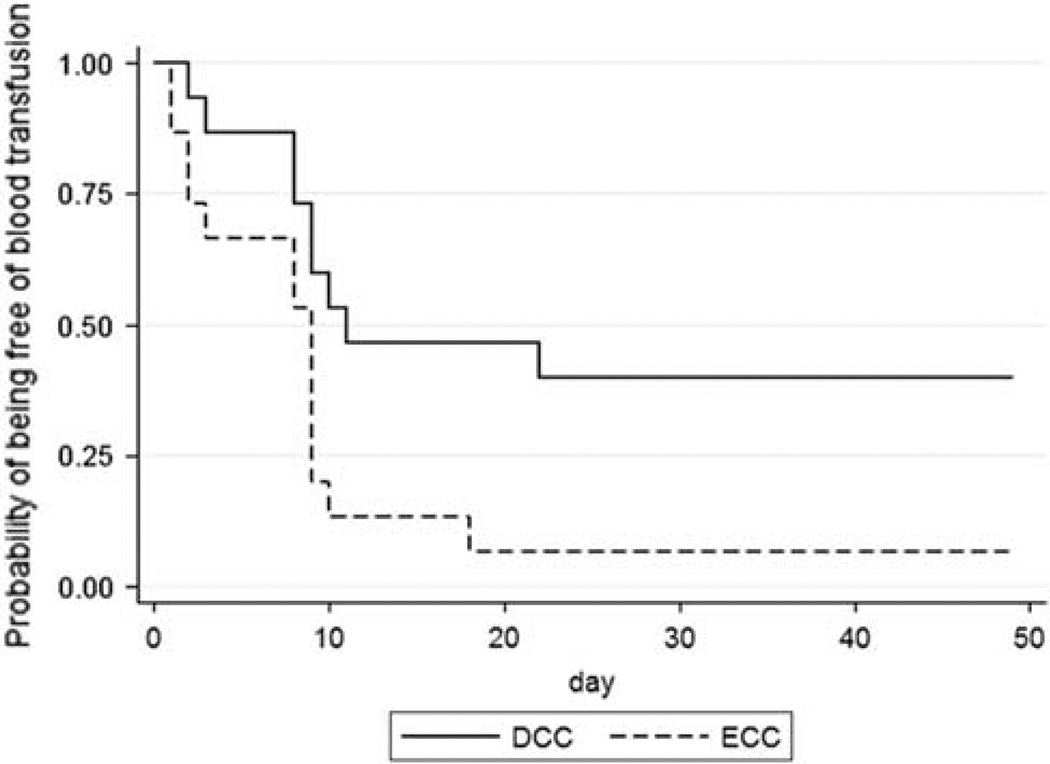
Results: Thirty infants were randomized at birth. No differences between the DCC and ECC groups were observed in gestational age at birth or time of surgery. No differences were observed across all safety measures, although a trend for higher peak serum bilirubin levels (9.2±2.2 vs 7.3±3.2 mg dl(-1), P=0.08) in the DCC group than in the ECC group was noted. Although similar at later time points, hematocrits were higher in the DCC than in the ECC infants during the first 72 h of life. The proportion of infants not receiving blood transfusions throughout hospitalization was higher in the DCC than in the ECC infants (43 vs 7%, log-rank test P=0.02).
Conclusion: DCC in infants with critical CHD appears both safe and feasible, with fewer infants exposed to red blood cell transfusions than with ECC. A more comprehensive appraisal of this practice is warranted.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Linderkamp O. Placental transfusion: determinants and effects. Clin Perinatol. 1982;9(3):559–592. - PubMed
-
- Usher R, Shephard M, Lind J. The blood volume of the newborn infant and placental transfusion. Acta Paediatr. 1963;52:497–512. - PubMed
-
- Yao AC, Lind J. Effect of gravity on placental transfusion. Lancet. 1969;2(7619):505–508. - PubMed
-
- Ceriani Cernadas JM, Carroli G, Pellegrini L, Otaño L, Ferreira M, Ricci C, et al. The effect of timing of cord clamping on neonatal venous hematocrit values and clinical outcome at term: a randomized, controlled trial. Pediatrics. 2006;117(4):e779–e786. - PubMed
-
- Nelle M, Kraus M, Bastert G, Linderkamp O. Effects of Leboyer childbirth on left-and right systolic time intervals in healthy term neonates. J Perinat Med. 1996;24(5):513–520. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
