

Risk factors for retained placenta
- PMID: 26226556
- PMCID: PMC10448481
- DOI: 10.1016/j.ajog.2015.07.039
Risk factors for retained placenta
Abstract
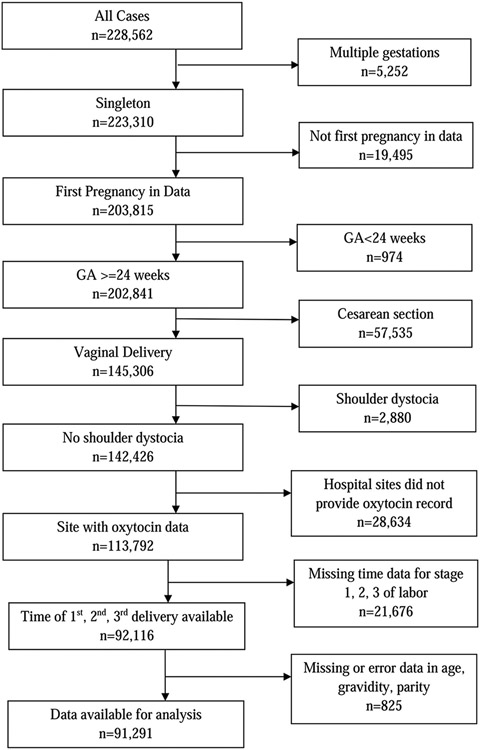
Objective: Retained placenta complicates 2-3% of vaginal deliveries and is a known cause of postpartum hemorrhage. Treatment includes manual or operative placental extraction, potentially increasing risks of hemorrhage, infections, and prolonged hospital stays. We sought to evaluate risk factors for retained placenta, defined as more than 30 minutes between the delivery of the fetus and placenta, in a large US obstetrical cohort.
Study design: We included singleton, vaginal deliveries ≥24 weeks (n = 91,291) from the Consortium of Safe Labor from 12 US institutions (2002-2008). Multivariable logistic regression analyses estimated the adjusted odds ratios (OR) and 95% confidence intervals (CI) for potential risk factors for retained placenta stratified by parity, adjusting for relevant confounding factors. Characteristics such as stillbirth, maternal age, race, and admission body mass index were examined.
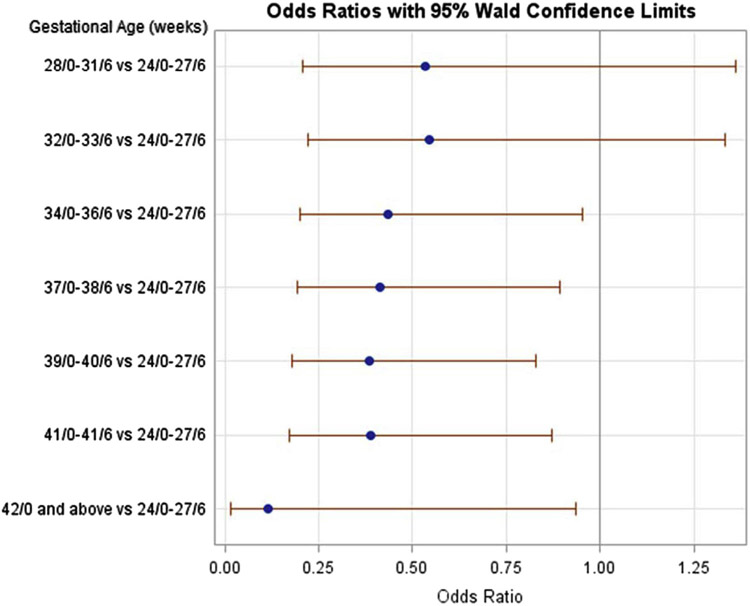
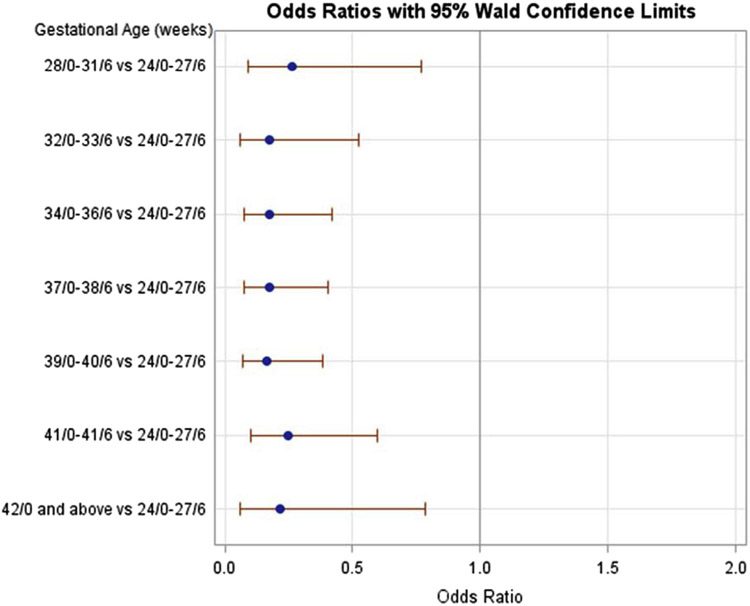
Results: Retained placenta complicated 1047 vaginal deliveries (1.12%). Regardless of parity, significant predictors of retained placenta included stillbirth (nulliparous adjusted OR, 5.67; 95% CI, 3.10-10.37; multiparous adjusted OR, 4.56; 95% CI, 2.08-9.94), maternal age ≥30 years, delivery at 24 0/7 to 27 6/7 compared with 34 weeks or later and delivery in a teaching hospital. In nulliparous women, additional risk factors were identified: longer first- or second-stage labor duration, whereas non-Hispanic black compared with non-Hispanic white race was found to be protective. Body mass index was not associated with an increased risk.
Conclusion: Multiple risk factors for retained placenta were identified, particularly the strong association with stillbirth. It is plausible that there could be something intrinsic about stillbirth that causes a retained placenta, or perhaps there are shared pathways of certain etiologies of stillbirth and a risk of retained placenta.
Keywords: postpartum hemorrhage; preterm birth; retained placenta; stillbirth.
Copyright © 2015 Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors report no conflict of interest.
Figures
References
-
- World Health Organization. WHO Recommendations for the prevention and treatment of postpartum haemorrhage. Geneva (Switzerland): World Health Organization; 2012. p.3. - PubMed
-
- Callahan WM, Kuklina EV, Berg CJ. Trends in postpartum hemorrhage: United States, 1994–2006. Am J Obstet Gynecol 2010;202:353. - PubMed
-
- National Collaborating Centre for Women’s and Children’s Health (NCCWCH). Intrapartum Care. Care of healthy women and their babies during childbirth. London (United Kingdom): RCOG Press; 2007. - PubMed
-
- World Health Organization. Pregnancy, childbirth, postpartum and newborn care: a guide for essential practice, 2nd ed. Geneva (Switzerland): World Health Organization; 2006. B11. - PubMed
-
- Combs CA, Laros RK. Prolonged third stage of labor: morbidity and risk factors. Obstet Gynecol 1991;77:863–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
