

High-Definition and Non-invasive Brain Modulation of Pain and Motor Dysfunction in Chronic TMD
- PMID: 26226938
- PMCID: PMC4656049
- DOI: 10.1016/j.brs.2015.06.008
High-Definition and Non-invasive Brain Modulation of Pain and Motor Dysfunction in Chronic TMD
Abstract
Background: Temporomandibular disorders (TMD) have a high prevalence and in many patients pain and masticatory dysfunction persist despite a range of treatments. Non-invasive brain neuromodulatory methods, namely transcranial direct current stimulation (tDCS), can provide relatively long-lasting pain relief in chronic pain patients.
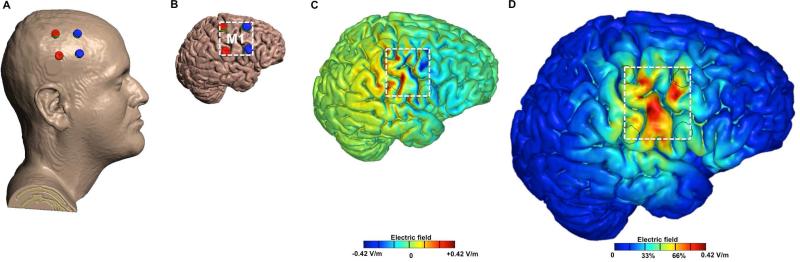
Objective: To define the neuromodulatory effect of five daily 2x2 motor cortex high-definition tDCS (HD-tDCS) sessions on clinical pain and motor measures in chronic TMD patients. It is predicted that M1 HD-tDCS will selectively modulate clinical measures, by showing greater analgesic after-effects compared to placebo, and active treatment will increase pain free jaw movement more than placebo.
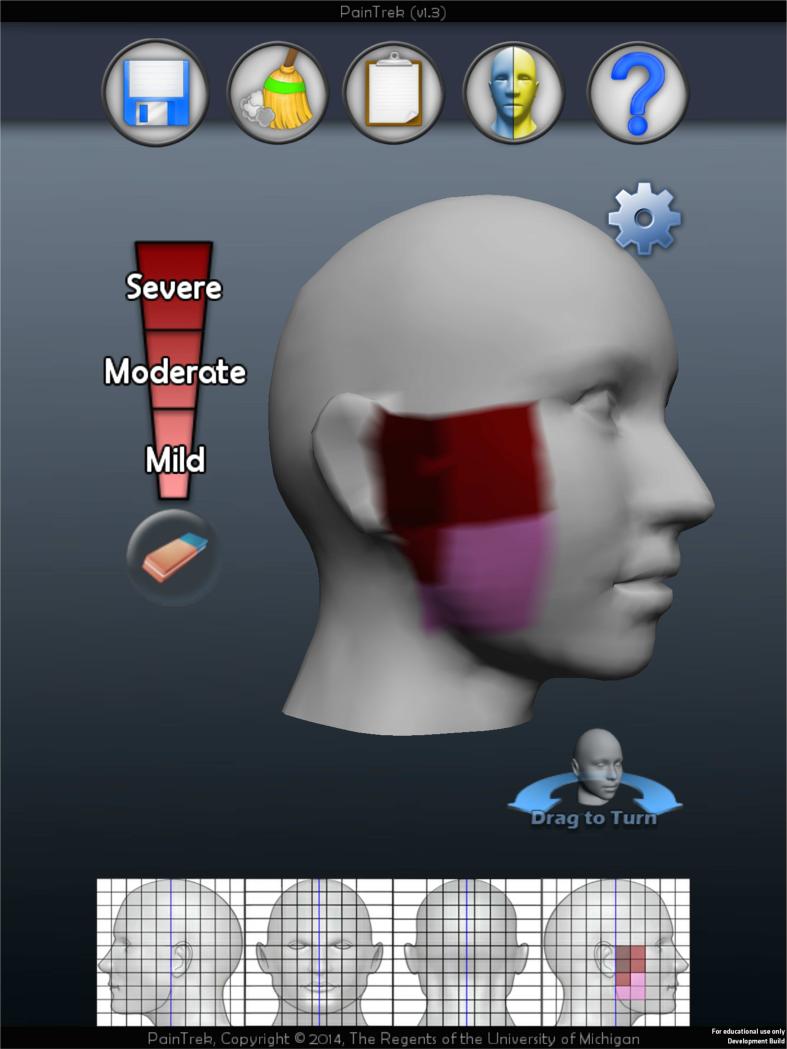
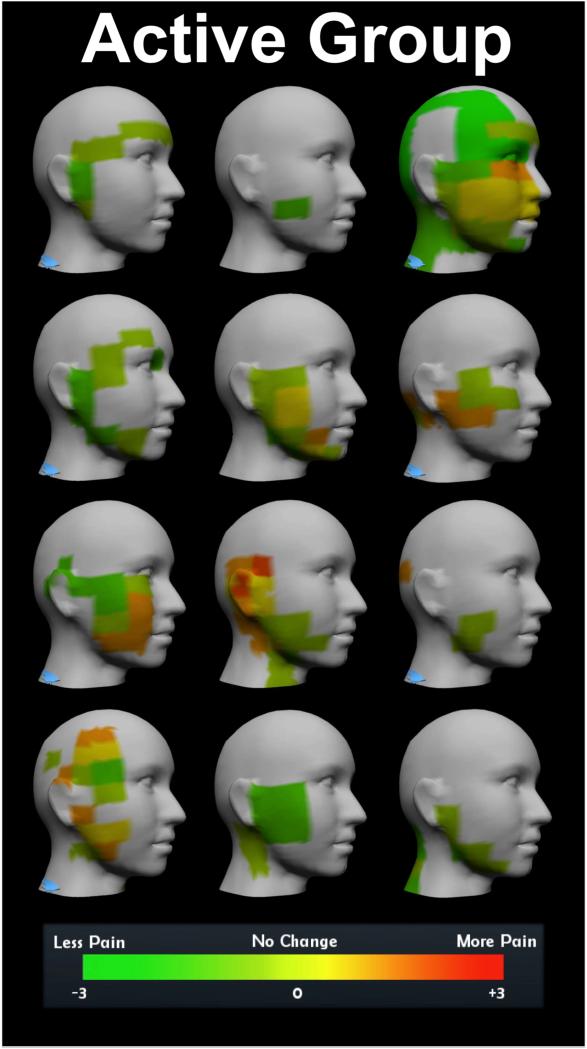
Methods: Twenty-four females with chronic myofascial TMD pain underwent five daily, 20-min sessions of active or sham 2 milliamps (mA) HD-tDCS. Measurable outcomes included pain-free mouth opening, visual analog scale (VAS), sectional sensory-discriminative pain measures tracked by a mobile application, short form of the McGill Pain Questionnaire, and the Positive and Negative Affect Schedule. Follow-up occurred at one-week and four-weeks post-treatment.
Results: There were significant improvements for clinical pain and motor measurements in the active HD-tDCS group compared to the placebo group for: responders with pain relief above 50% in the VAS at four-week follow-up (P = 0.04); pain-free mouth opening at one-week follow-up (P < 0.01); and sectional pain area, intensity and their sum measures contralateral to putative M1 stimulation during the treatment week (P < 0.01). No changes in emotional values were shown between groups.
Conclusion: Putative M1 stimulation by HD-tDCS selectively improved meaningful clinical sensory-discriminative pain and motor measures during stimulation, and up to four-weeks post-treatment in chronic myofascial TMD pain patients.
Keywords: Clinical trial; Pain; PainTrek; Temporomandibular disorder; Transcranial direct current stimulation.
Copyright © 2015 Elsevier Inc. All rights reserved.
Figures
References
-
- LeResche L. Epidemiology of temporomandibular disorders: implications for the investigation of etiologic factors. Crit Rev Oral Biol Med. 1997;8(3):291–305. - PubMed
-
- Lipton JA, Ship JA, Larach-Robinson D. Estimated prevalence and distribution of reported orofacial pain in the United States. J Am Dent Assoc. 1993 Oct;124(10):115–21. - PubMed
-
- Woolf CJ, Ma Q. Nociceptors--noxious stimulus detectors. Neuron. 2007 Aug 2;55(3):353–64. - PubMed
-
- Lima MC, Fregni F. Motor cortex stimulation for chronic pain: systematic review and meta-analysis of the literature. Neurology. 2008 Jun 10;70(24):2329–37. - PubMed
-
- Tsubokawa T, Katayama Y, Yamamoto T, Hirayama T, Koyama S. Chronic motor cortex stimulation for the treatment of central pain. Acta Neurochir Suppl (Wien) 1991;52:137–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
