

Cardiac Stem Cell Hybrids Enhance Myocardial Repair
- PMID: 26228030
- PMCID: PMC4583815
- DOI: 10.1161/CIRCRESAHA.115.306838
Cardiac Stem Cell Hybrids Enhance Myocardial Repair
Abstract
Rationale: Dual cell transplantation of cardiac progenitor cells (CPCs) and mesenchymal stem cells (MSCs) after infarction improves myocardial repair and performance in large animal models relative to delivery of either cell population.
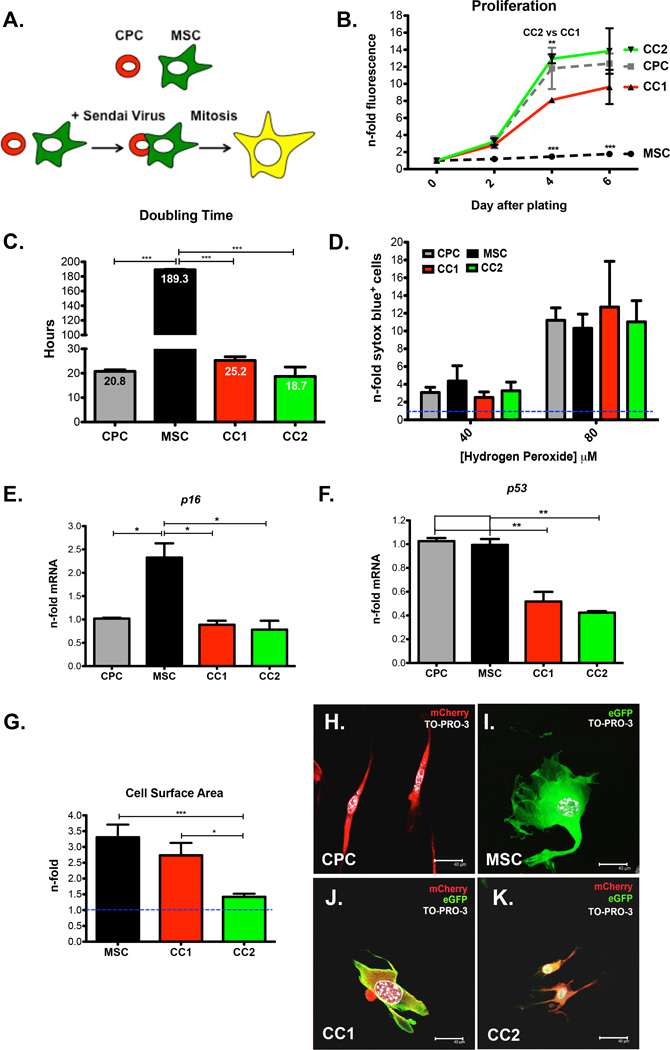
Objective: To demonstrate that CardioChimeras (CCs) formed by fusion between CPCs and MSCs have enhanced reparative potential in a mouse model of myocardial infarction relative to individual stem cells or combined cell delivery.
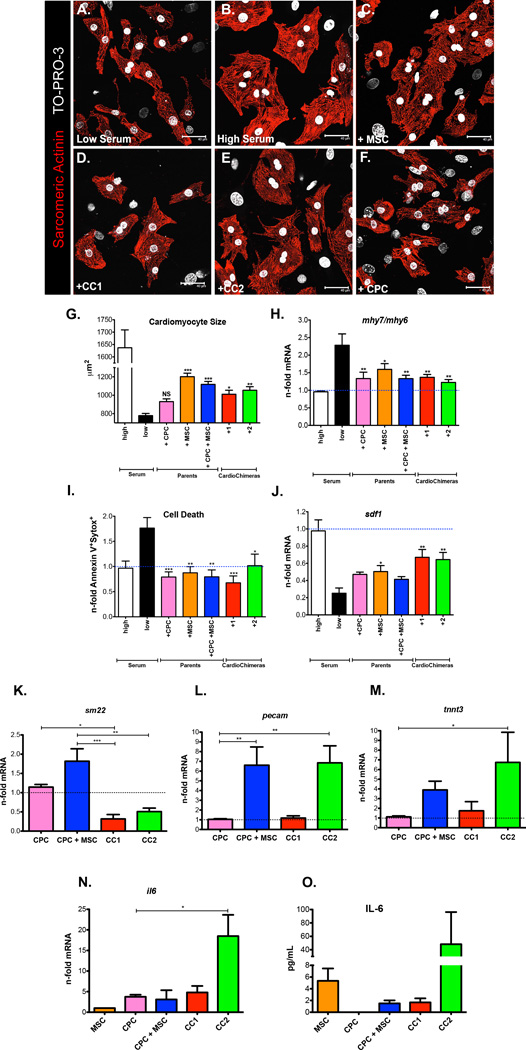
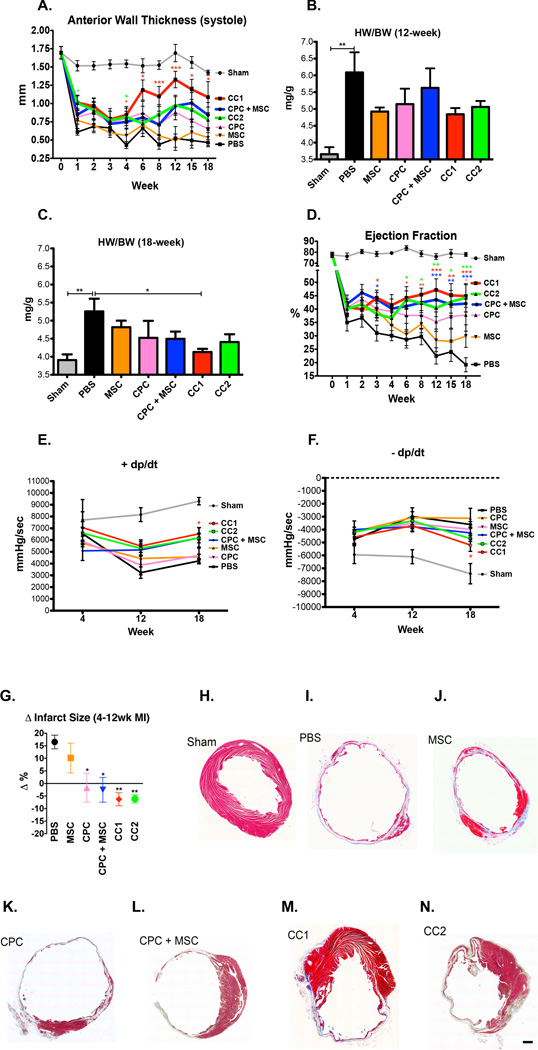
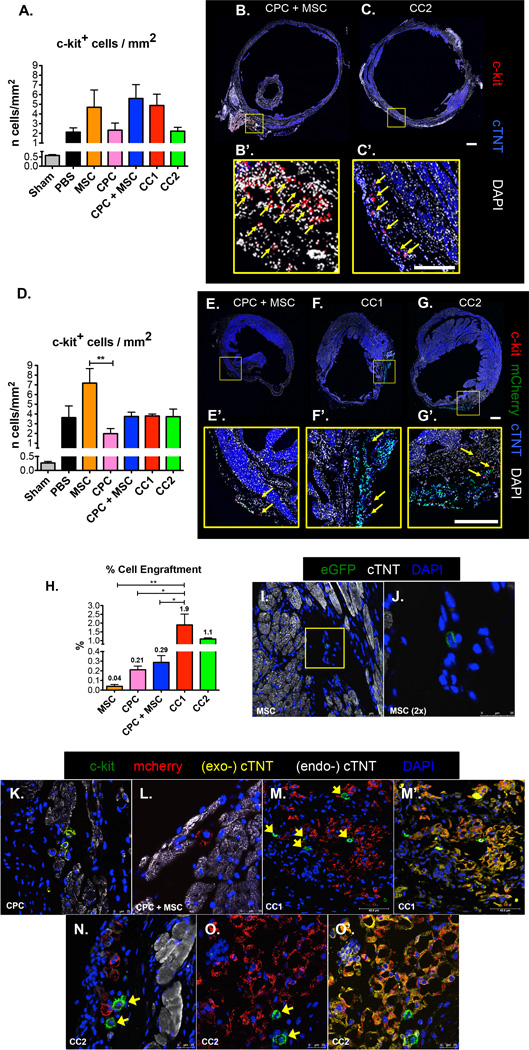
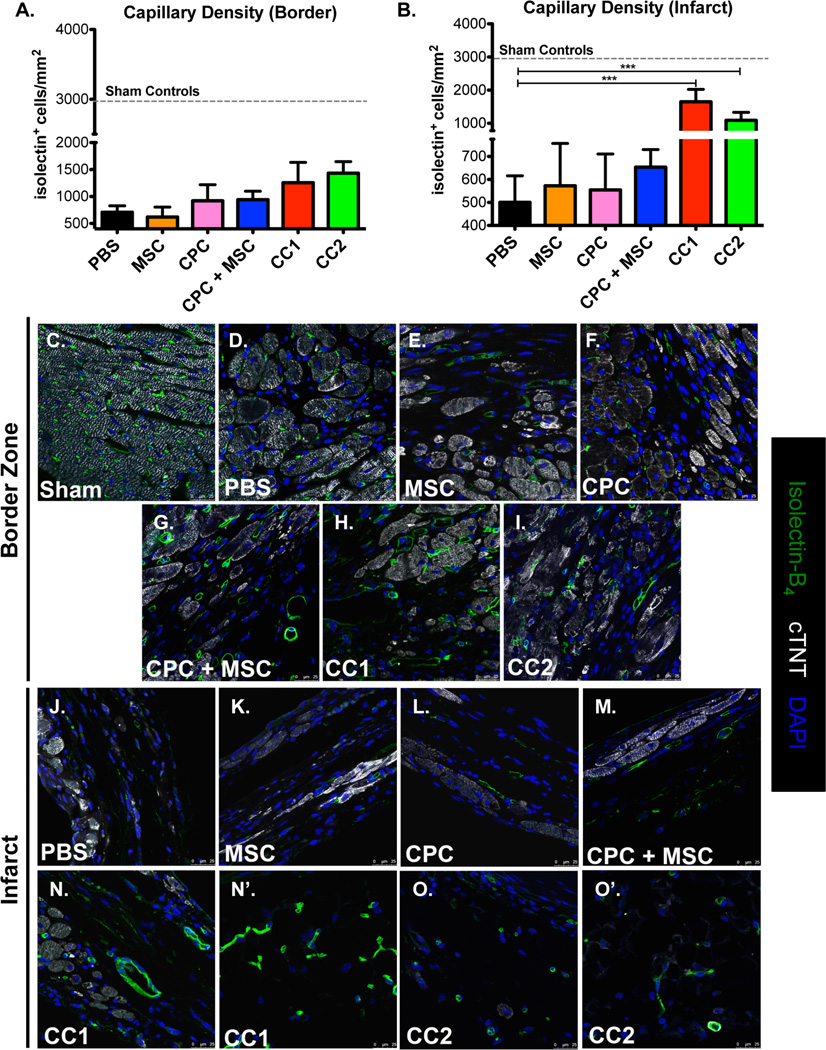
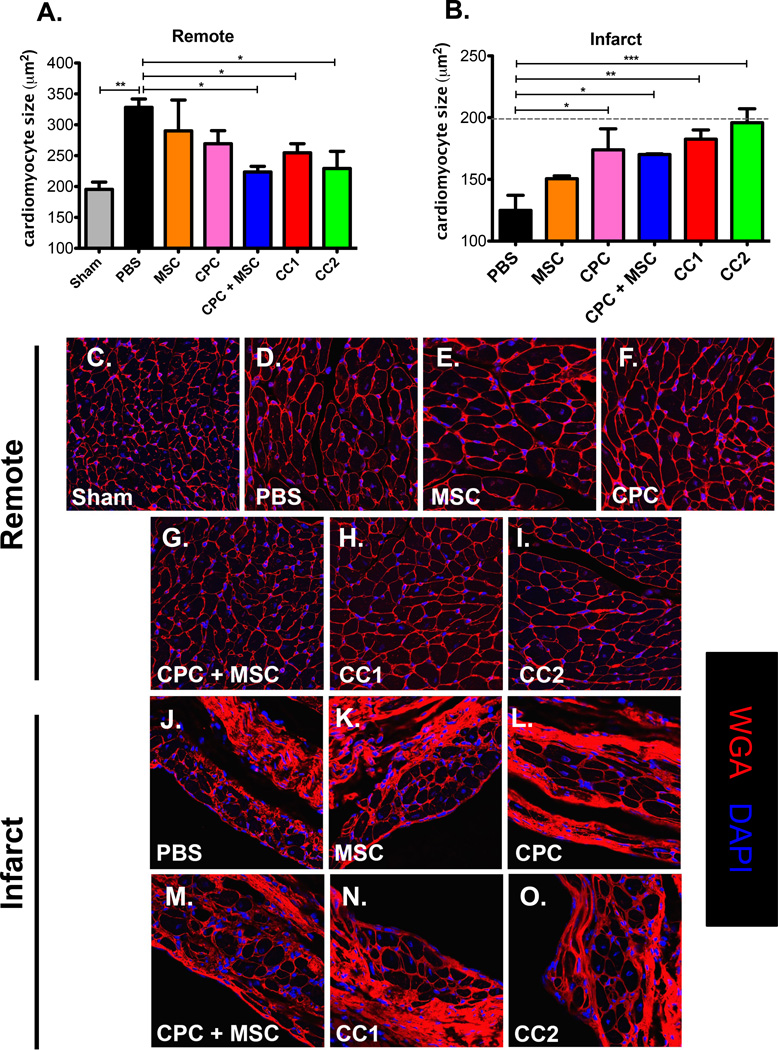
Methods and results: Two distinct and clonally derived CCs, CC1 and CC2, were used for this study. CCs improved left ventricular anterior wall thickness at 4 weeks post injury, but only CC1 treatment preserved anterior wall thickness at 18 weeks. Ejection fraction was enhanced at 6 weeks in CCs, and functional improvements were maintained in CCs and CPC+MSC groups at 18 weeks. Infarct size was decreased in CCs, whereas CPC+MSC and CPC parent groups remained unchanged at 12 weeks. CCs exhibited increased persistence, engraftment, and expression of early commitment markers within the border zone relative to combinatorial and individual cell population-injected groups. CCs increased capillary density and preserved cardiomyocyte size in the infarcted regions suggesting CCs role in protective paracrine secretion.
Conclusions: CCs merge the application of distinct cells into a single entity for cellular therapeutic intervention in the progression of heart failure. CCs are a novel cell therapy that improves on combinatorial cell approaches to support myocardial regeneration.
Keywords: cell fusion; mesenchymal stromal cells; myocardial infarction; myocytes, cardiac; stem cells.
© 2015 American Heart Association, Inc.
Figures
Comment in
-
Cell Therapy: Targeting Endogenous Repair Versus Remuscularization.Circ Res. 2015 Sep 25;117(8):659-61. doi: 10.1161/CIRCRESAHA.115.307346. Circ Res. 2015. PMID: 26405181 Free PMC article. No abstract available.
References
-
- Hong KU, Guo Y, Li QH, Cao P, Al-Maqtari T, Vajravelu BN, Du J, Book MJ, Zhu X, Nong Y, Bhatnagar A, Bolli R. C-kit+ cardiac stem cells alleviate post-myocardial infarction left ventricular dysfunction despite poor engraftment and negligible retention in the recipient heart. PLoS One. 2014;9:e96725. - PMC - PubMed
-
- Mohsin S, Khan M, Toko H, Bailey B, Cottage CT, Wallach K, Nag D, Lee A, Siddiqi S, Lan F, Fischer KM, Gude N, Quijada P, Avitabile D, Truffa S, Collins B, Dembitsky W, Wu JC, Sussman MA. Human cardiac progenitor cells engineered with pim-i kinase enhance myocardial repair. Journal of the American College of Cardiology. 2012;60:1278–1287. - PMC - PubMed
-
- Leri A, Kajstura J, Anversa P. Cardiac stem cells and mechanisms of myocardial regeneration. Physiological reviews. 2005;85:1373–1416. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01 HL122525/HL/NHLBI NIH HHS/United States
- R01 HL105759/HL/NHLBI NIH HHS/United States
- F31 HL117623/HL/NHLBI NIH HHS/United States
- P01HL085577/HL/NHLBI NIH HHS/United States
- R01HL067245/HL/NHLBI NIH HHS/United States
- F31HL117623/HL/NHLBI NIH HHS/United States
- R37 HL091102/HL/NHLBI NIH HHS/United States
- R37HL091102/HL/NHLBI NIH HHS/United States
- R01 HL113647/HL/NHLBI NIH HHS/United States
- R01HL105759/HL/NHLBI NIH HHS/United States
- R01HL113647/HL/NHLBI NIH HHS/United States
- R01HL117163/HL/NHLBI NIH HHS/United States
- R01 HL067245/HL/NHLBI NIH HHS/United States
- R01 HL113656/HL/NHLBI NIH HHS/United States
- R01 HL117163/HL/NHLBI NIH HHS/United States
- R01HL122525/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
