

Carotid Webs and Recurrent Ischemic Strokes in the Era of CT Angiography
- PMID: 26228877
- PMCID: PMC7964886
- DOI: 10.3174/ajnr.A4431
Carotid Webs and Recurrent Ischemic Strokes in the Era of CT Angiography
Abstract
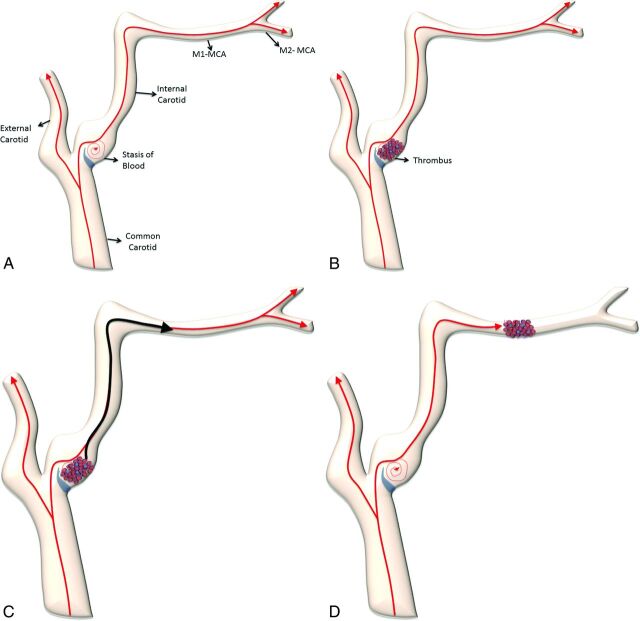
Background and purpose: Carotid webs may cause recurrent ischemic stroke. We describe the prevalence, demographics, clinical presentation, imaging features, histopathology, and stroke risk associated with this under-recognized lesion.
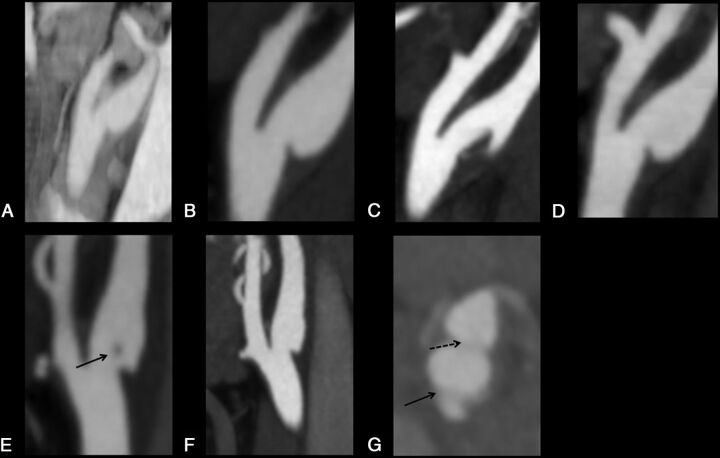
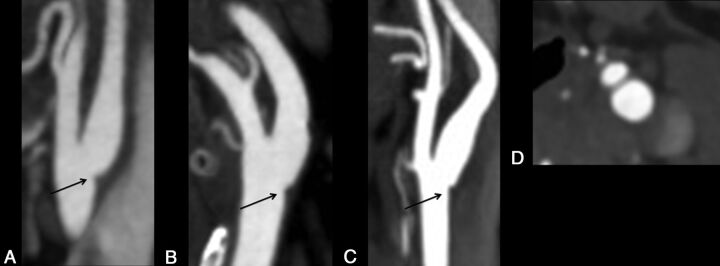
Materials and methods: A carotid web was defined on CTA as a thin intraluminal filling defect along the posterior wall of the carotid bulb just beyond the carotid bifurcation on oblique sagittal section CTA that was seen as a septum on axial CTA. Using a prospective case series from April 2013 to April 2014, we describe the demographics, spectrum of imaging features on CTA, and histopathology of these carotid webs. From a retrospective analysis of patients at our center from May 2012 to April 2013 who had a baseline head and neck CTA followed by a brain MR imaging within 1-2 days of the CTA, we determine the period prevalence of carotid webs and the prevalence of ipsilateral stroke on imaging.
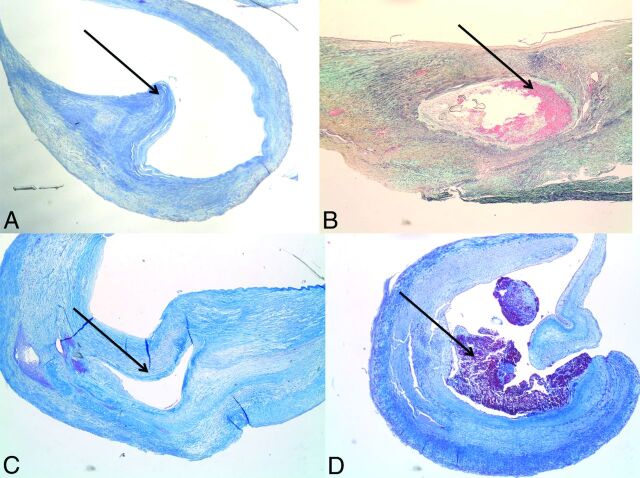
Results: In the prospective series, the mean age was 50 years (range, 41-55 years); 5/7 patients were women. Recurrent stroke was seen in 5/7 (71.4%) patients with the carotid web; time to recurrence ranged from 1 to 97 months. Histopathology suggested a high probability of fibromuscular dysplasia. In the retrospective series, carotid webs were seen in 7/576 patients for a hospital-based-period prevalence of 1.2% (95% CI, 0.4%-2.5%). Two of these 7 patients had acute stroke in the vascular territory of the carotid web.
Conclusions: A carotid web may contribute to recurrent ischemic stroke in patients with no other determined stroke mechanism. Intimal variant fibromuscular dysplasia is the pathologic diagnosis in most cases. The prevalence of carotid web is low, while the optimal management strategy remains unknown.
© 2015 by American Journal of Neuroradiology.
Figures
Comment in
-
Carotid Web: Appearance at MR Angiography.AJNR Am J Neuroradiol. 2016 Jan;37(1):E5-6. doi: 10.3174/ajnr.A4598. Epub 2015 Oct 15. AJNR Am J Neuroradiol. 2016. PMID: 26471750 Free PMC article. No abstract available.
References
-
- Karlson KJ, Wolf B, Neptune WB. Symptomatic carotid stenosis secondary to an intraluminal web: a case report. Vasc Endovascular Surg 1987;21:422–26 10.1177/153857448702100609 - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous