

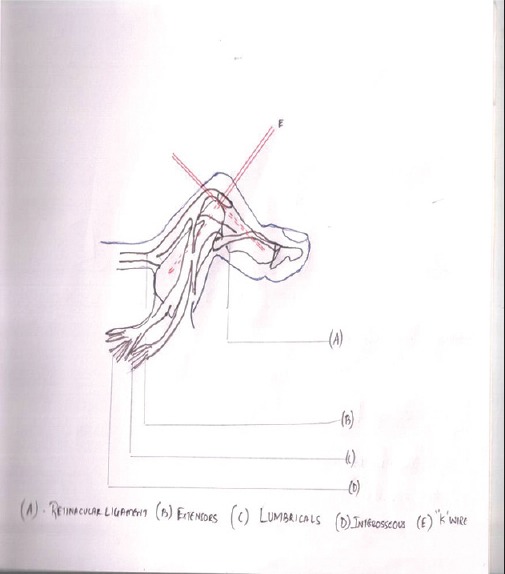
Safe corridors for K-wiring in phalangeal fractures
- PMID: 26229157
- PMCID: PMC4510790
- DOI: 10.4103/0019-5413.159591
Safe corridors for K-wiring in phalangeal fractures
Abstract
Background: Unstable phalangeal fractures are commonly treated with K-wire fixation. Operative fixation must be used judiciously and with the expectation that the ultimate outcome should be better than the outcome after nonoperative management. It is necessary to achieve a stable fracture fixation and early mobilization. In order to achieve this goal, one should closely understand the safe portals/corridors in hand for K-wire entry for fractures of the phalanges. Safe corridors were defined and tested using a pilot cadaveric and a clinical case study by assessing the outcome.
Materials and methods: In our prospective case series, 50 patients with 64 phalangeal fractures were treated with closed reduction and K-wires were inserted through safe portals identified by a pilot cadaveric study. On table active finger movement test was done and the results were analyed using radiology, disabilities of the arm, shoulder, and hand (DASH) score and total active motion (TAM). In our study, little finger (n = 28) was the most commonly involved digit. In fracture pattern, transverse (n = 20) and spiral (n = 20) types were common. Proximal phalanx (n = 38) was commonly involved and the common site being the base of the phalanx (n = 28).
Results: 47 (95%) patients had excellent TAM and the mean postoperative DASH score was 58.05. All patients achieved excellent and good scores proving the importance of the safe corridor concept.
Conclusion: K-wiring through the safe corridor has proved to yield the best clinical results because of least tethering of soft tissues as evidenced by performing "on-table active finger movement test" at the time of surgery. We strongly recommend K-wiring through safe portals in all phalangeal fractures.
Keywords: K-wire; Phalanges of fingers; fracture fixation; fractures; hand injuries; metacarpo-phalangeal joint; phalanges; proximal interphalangeal joint.
Conflict of interest statement
Figures







References
-
- Stern PJ. Fractures of metacarpals and phalanges. In: Green DP, Hotchkiss RN, Pederson WC, editors. Green's Operative Hand Surgery. 4th ed. Vol. 1. Churchill Livingstone: Philadelphia US; 1999. pp. 711–57.
-
- Watson-Jones R, Barton NJ. Fractures and joint injuries of the hand. In: Wilson JN, editor. Watson-Jones Fractures and Joint Injuries. 7th ed. Noida: Elsevier Publishers; 2009. pp. 650–95.
-
- Barton N. Internal fixation of the hand. J Hand Surg Br. 1989;14:139–42. - PubMed
-
- Margic K. External fixation of closed metacarpal and phalangeal fractures of digits. A prospective study of one hundred consecutive patients. J Hand Surg Br. 2006;31:30–40. - PubMed
-
- Hudak PL, Amadio PC, Bombardier C. Development of an upper extremity outcome measure: The DASH (disabilities of the arm, shoulder and hand) [corrected] The Upper Extremity Collaborative Group (UECG) Am J Ind Med. 1996;29:602–8. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources