

Hepatic inflammatory pseudotumor presenting in an 8-year-old boy: A case report and review of literature
- PMID: 26229415
- PMCID: PMC4515854
- DOI: 10.3748/wjg.v21.i28.8730
Hepatic inflammatory pseudotumor presenting in an 8-year-old boy: A case report and review of literature
Abstract
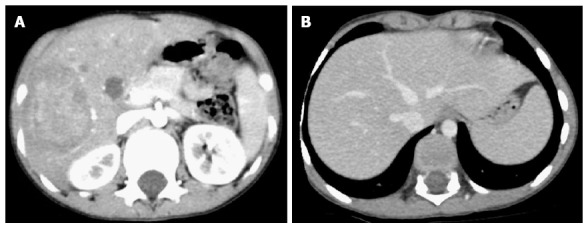
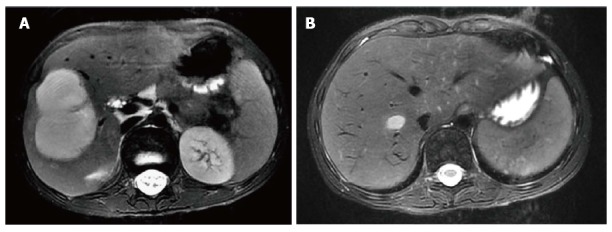
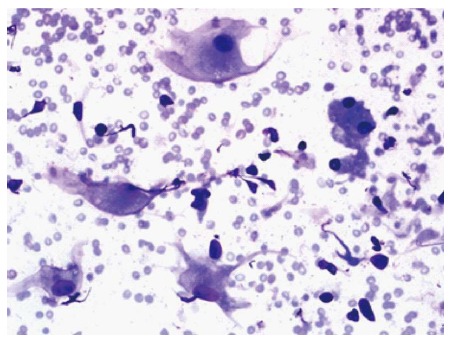
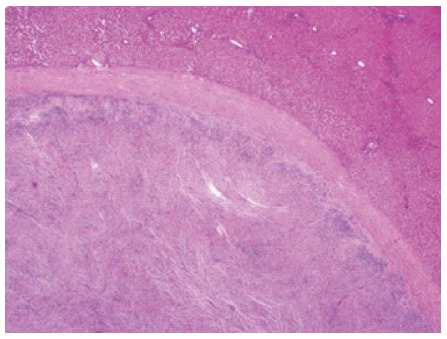
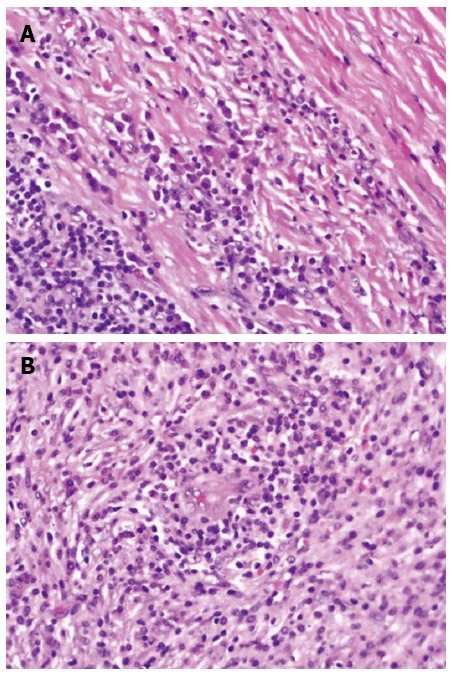
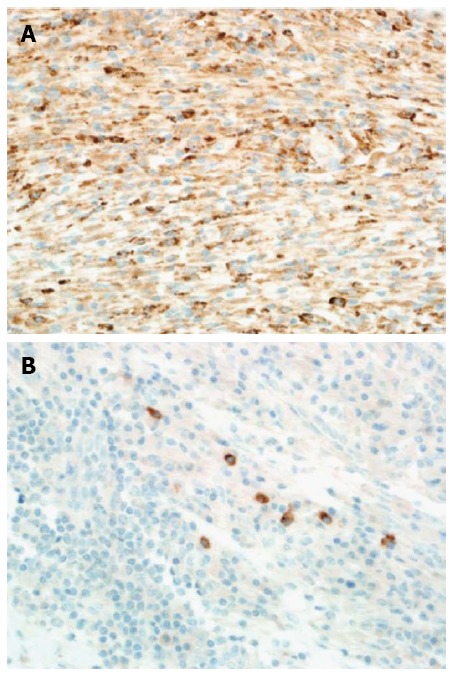
Hepatic inflammatory pseudotumors are uncommon benign lesions. Accurately diagnosing hepatic inflammatory pseudotumor can be very challenging because the clinical presentation and radiological appearances are nonspecific and cannot be certainly distinguished from malignant neoplastic processes. Herein, we present a case of hepatic IPT in an 8-year-old boy who presented to clinic with a 3-mo history of a tender hepatic mass, fever of unknown origin, and 9-kg weight loss. The physical examination was notable for tender hepatomegaly. Laboratory investigations were notable for a normal hepatic profile and elevated erythrocyte sedimentation rate and C-reactive protein. A T2-attenuated magnetic resonance imaging scan of the abdomen showed a 4.7 cm × 4.7 cm × 6.6 cm, contrast-enhancing, hyper-intense, well-defined lesion involving the right hepatic lobe. In view of the unremitting symptoms, tender hepatomegaly, thrombosed right hepatic vein, nonspecific radiological findings, and high suspicion of a deep-seated underlying infection or malignancy, a right hepatic lobectomy was recommended. Microscopically, the hepatic lesion exhibited a mixture of inflammatory cells (histiocytes, plasma cells, mature lymphocytes, and occasional multinucleated giant cells) in a background of dense fibrous tissue. Immunohistochemically, the cells stained negative for SMA, ALK-1, CD-21 and CD-23, diffusely positive for CD-68, and focally positive for IgG4. The final histopathological diagnosis was consistent with hepatic IPT. At the postoperative 4-mo follow-up, the patient was asymptomatic without radiological evidence of recurrence.
Keywords: Hepatic; Inflammatory myofibroblastic tumor; Inflammatory pseudotumor; Liver.
Figures

References
-
- Souid AK, Ziemba MC, Dubansky AS, Mazur M, Oliphant M, Thomas FD, Ratner M, Sadowitz PD. Inflammatory myofibroblastic tumor in children. Cancer. 1993;72:2042–2048. - PubMed
-
- Melloni G, Carretta A, Ciriaco P, Arrigoni G, Fieschi S, Rizzo N, Bonacina E, Augello G, Belloni PA, Zannini P. Inflammatory pseudotumor of the lung in adults. Ann Thorac Surg. 2005;79:426–432. - PubMed
-
- Coffin CM, Humphrey PA, Dehner LP. Extrapulmonary inflammatory myofibroblastic tumor: a clinical and pathological survey. Semin Diagn Pathol. 1998;15:85–101. - PubMed
-
- Nagarajan S, Jayabose S, McBride W, Prasadh I, Tanjavur V, Marvin MR, Rodriguez-Davalos MI. Inflammatory myofibroblastic tumor of the liver in children. J Pediatr Gastroenterol Nutr. 2013;57:277–280. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
