

Maternal ophthalmic artery Doppler velocimetry in pre-eclampsia in Southwestern Nigeria
- PMID: 26229508
- PMCID: PMC4514353
- DOI: 10.2147/IJWH.S86314
Maternal ophthalmic artery Doppler velocimetry in pre-eclampsia in Southwestern Nigeria
Abstract
Background: Pre-eclampsia (PE) poses a serious challenge to maternal and fetal health in Africa. It is associated with hemodynamic changes that may affect the internal carotid/ophthalmic artery circulation with consequent neuro-ophthalmic manifestations. Ophthalmic artery Doppler (OAD) ultrasound is an important tool that can be used to detect hemodynamic changes in PE and monitor its severity. In this study, we evaluated hemodynamic changes on OAD ultrasound in the ophthalmic arteries of pre-eclamptic women and compared these with values in healthy pregnant women.
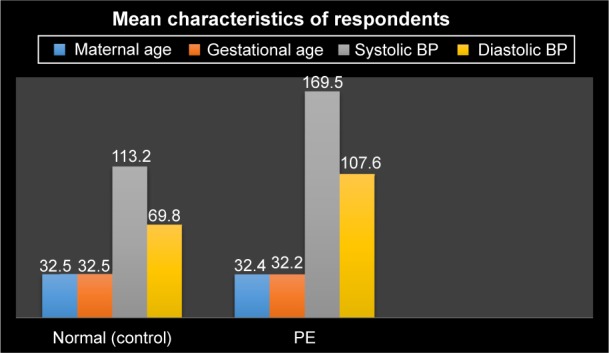
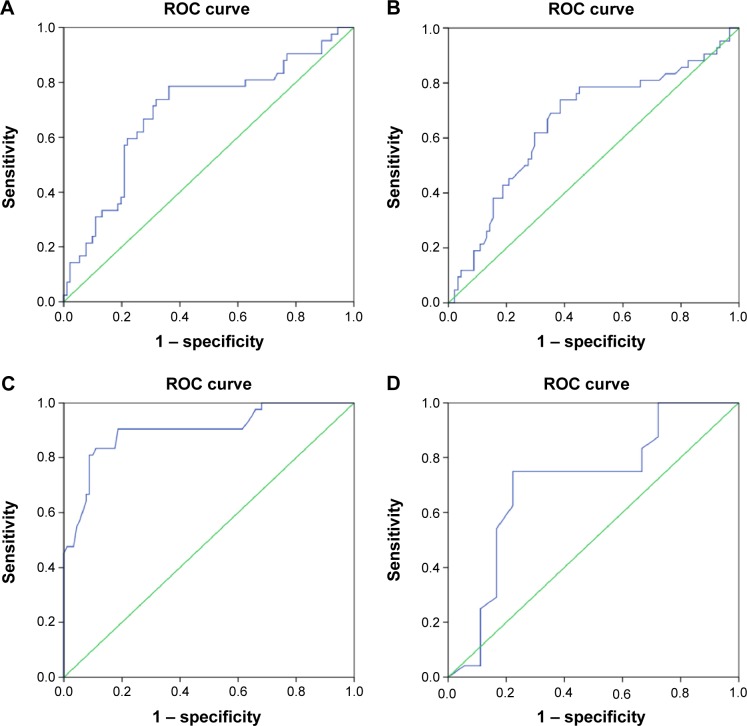
Methods: OAD parameters, such as, peak systolic velocity, peak diastolic velocity, end diastolic velocity, pulsatility index, and peak ratio, were measured on transorbital triplex ultrasound scan with a 7-10 MHz multifrequency linear transducer in 42 consenting pre-eclamptic patients and 41 pregnant controls matched for maternal age, gestational age, and parity at the Department of Radiology, University College Hospital, Ibadan. Univariate, bivariate, and receiver operating characteristic curve data analyses were performed. P<0.05 was considered to be statistically significant.
Results: Mean resistivity index, pulsatility index, and peak systolic velocity were significantly lower in pre-eclamptic patients than in the controls. Mean peak diastolic velocity, end diastolic velocity, and peak ratio were significantly higher in the pre-eclamptic group. The receiver operating characteristic curve showed that the resistivity index (sensitivity 75%, specificity 77.8%) could distinguish mild from severe PE while the peak ratio (sensitivity 90.5%, specificity 81.3%) could accurately detect PE.
Conclusion: OAD ultrasound can be used to monitor patients with PE for early detection of progression to severe forms before cerebral complications develop. OAD screening of patients at high risk for PE can also detect early changes of hemodynamic derangement.
Keywords: Doppler parameters; hemodynamic changes; ophthalmic artery; ultrasound.
Figures



References
-
- Tamas P, Hantosi E, Bodis J. Hypertensive disorders of pregnancy: theory of hypoperfusion and hyperperfusion types of pre-eclampsia. Gynaecol Perinatol. 2010;19:255–260.
-
- World Health Organization Global program to conquer pre-eclampsia/eclampsia. 2002. [Accessed June 18, 2015]. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3087154/
-
- Shah A, Fawole B, M’ Imunya JM, et al. Cesarean delivery outcomes from the WHO global survey on maternal and perinatal health in Africa. Int J Gynaecol Obstet. 2009;107:191–197. - PubMed
LinkOut - more resources
Full Text Sources
