

Effects of dexmedetomidine and clonidine as propofol adjuvants on intra-operative hemodynamics and recovery profiles in patients undergoing laparoscopic cholecystectomy: A prospective randomized comparative study
- PMID: 26229757
- PMCID: PMC4510823
- DOI: 10.4103/2231-0770.160231
Effects of dexmedetomidine and clonidine as propofol adjuvants on intra-operative hemodynamics and recovery profiles in patients undergoing laparoscopic cholecystectomy: A prospective randomized comparative study
Abstract
Context: Alpha-2 (α2) adrenergic receptor agonists, clonidine and dexmedetomidine, are widely used as adjuvants during anesthesia for analgesic, sedative, sympatholytic, and cardiovascular stabilizing effects.
Aims: We compared effects of clonidine and dexmedetomidine (as propofol adjuvants) on intra-operative hemodynamics, recovery time, and postoperative cognitive function impairment.
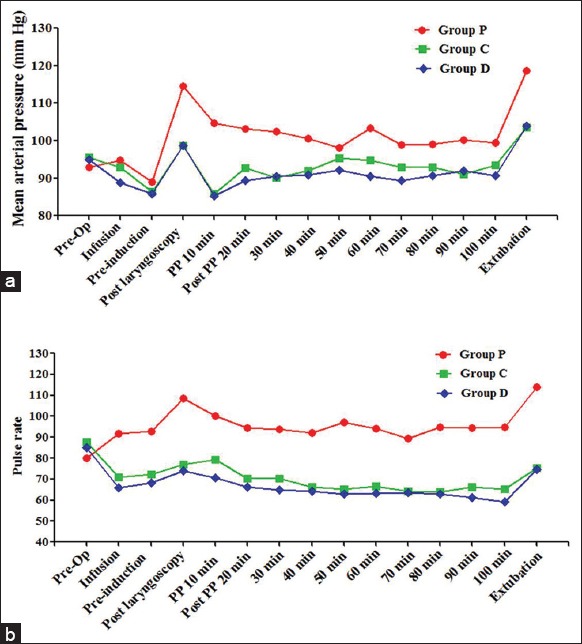
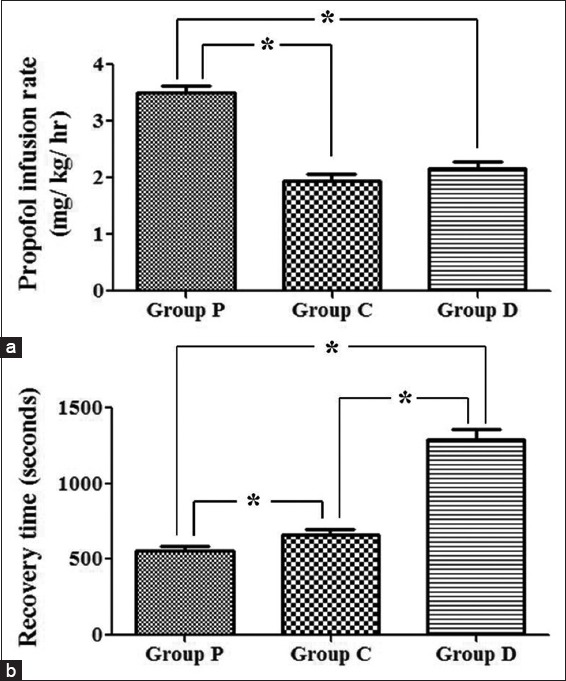
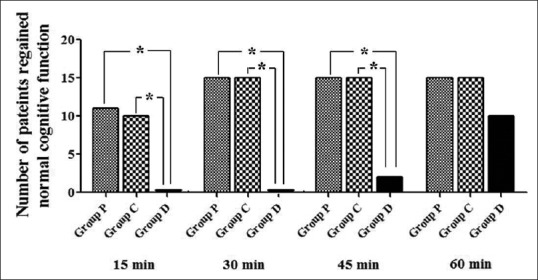
Subjects and methods: Forty-five American Society of Anesthesiologists I and II patients, scheduled for laparoscopic cholecystectomy were divided into three groups (n = 15). Group C patients received bolus of clonidine 3 μg/kg followed by a continuous infusion; Group D patients received dexemedetomidine 1 μg/kg and a continuous infusion; and Group P patients received a bolus of normal saline followed by an infusion. Intra-operative mean arterial pressure (MAP) and pulse rate (PR) were measured throughout the surgery. Bispectral index was maintained at 55 ± 5 by titrating propofol infusion rate. The time between the interruption of anesthesia and eye opening (recovery time) was measured. Cognitive function was assessed using short mental status questionnaire at 15, 30, 45, and 60 min postoperatively.
Results: The sympathetic response to laryngoscopy and extubation on MAP and PR were significantly reduced with the use of clonidine and dexmedetomidine (P < 0.05). The recovery was delayed (P < 0.05) with both the drug combinations and it was more pronounced with dexmedetomidine (P < 0.05). Dexmedetomidine group showed cognitive impairment in a postoperative period lasting up to an hour.
Conclusions: When co-administered with propofol, both clonidine, and dexmedetomidine attenuate sympathetic response to laryngoscopy and extubation but cause delay in the recovery from anesthesia. Dexmedetomidine causes impairment of postoperative cognitive functions.
Keywords: Clonidine; cognitive dysfunction; dexmedetomidine; hemodynamics; recovery time.
Figures
References
-
- Kulka PJ, Tryba M, Zenz M. Dose-response effects of intravenous clonidine on stress response during induction of anesthesia in coronary artery bypass graft patients. Anesth Analg. 1995;80:263–8. - PubMed
-
- De Kock M, Crochet B, Morimont C, Scholtes JL. Intravenous or epidural clonidine for intra- and postoperative analgesia. Anesthesiology. 1993;79:525–31. - PubMed
-
- Ma D, Rajakumaraswamy N, Maze M. alpha2-adrenoceptor agonists: Shedding light on neuroprotection? Br Med Bull. 2004;71:77–92. - PubMed
-
- Ohtani N, Kida K, Shoji K, Yasui Y, Masaki E. Recovery profiles from dexmedetomidine as a general anesthetic adjuvant in patients undergoing lower abdominal surgery. Anesth Analg. 2008;107:1871–4. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials