

Exercise training improves peak oxygen consumption and haemodynamics in patients with severe pulmonary arterial hypertension and inoperable chronic thrombo-embolic pulmonary hypertension: a prospective, randomized, controlled trial
- PMID: 26231884
- PMCID: PMC4692286
- DOI: 10.1093/eurheartj/ehv337
Exercise training improves peak oxygen consumption and haemodynamics in patients with severe pulmonary arterial hypertension and inoperable chronic thrombo-embolic pulmonary hypertension: a prospective, randomized, controlled trial
Abstract
Aims: The impact of exercise training on the right heart and pulmonary circulation has not yet been invasively assessed in patients with pulmonary hypertension (PH) and right heart failure. This prospective randomized controlled study investigates the effects of exercise training on peak VO2/kg, haemodynamics, and further clinically relevant parameters in PH patients.
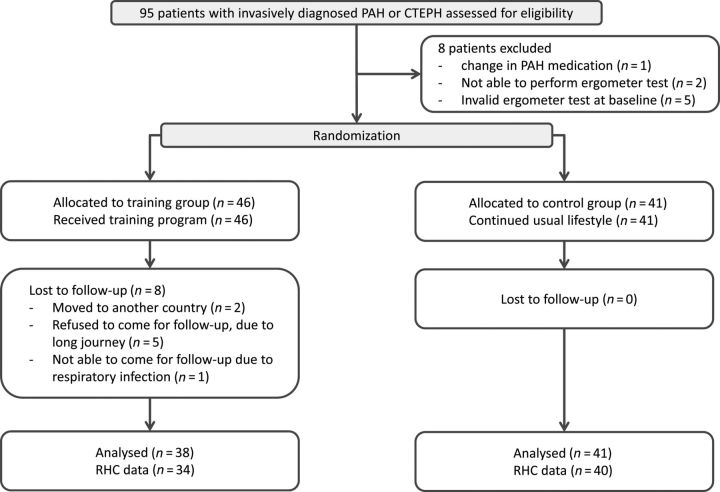
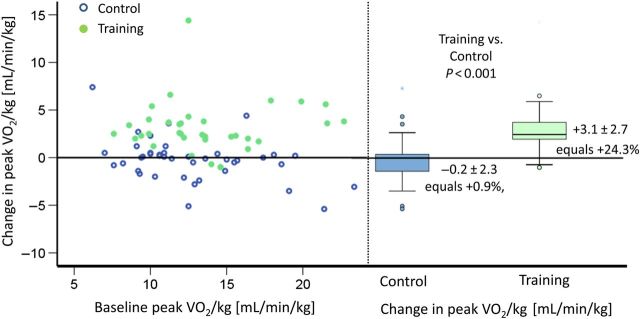
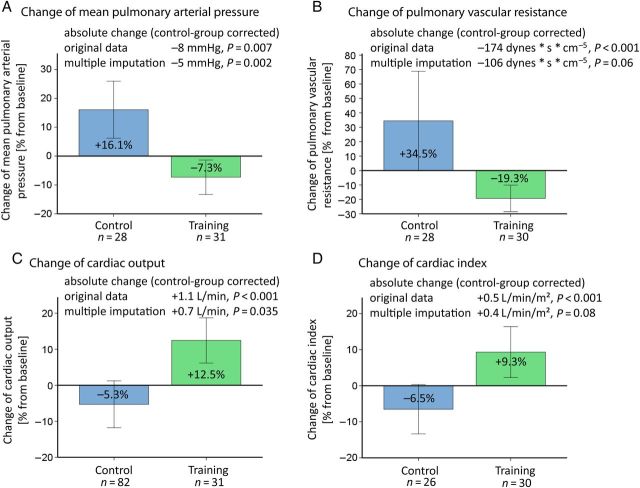
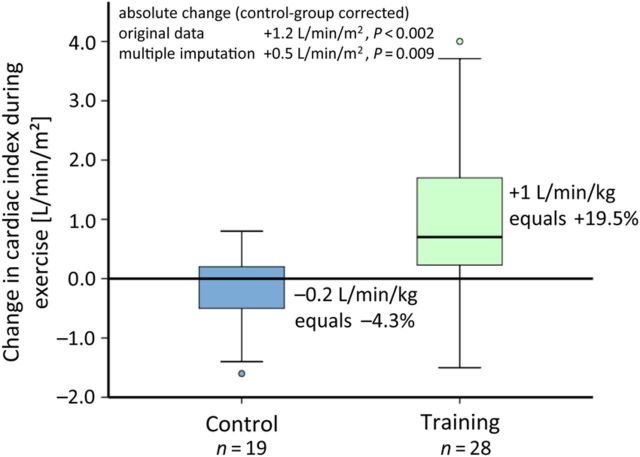
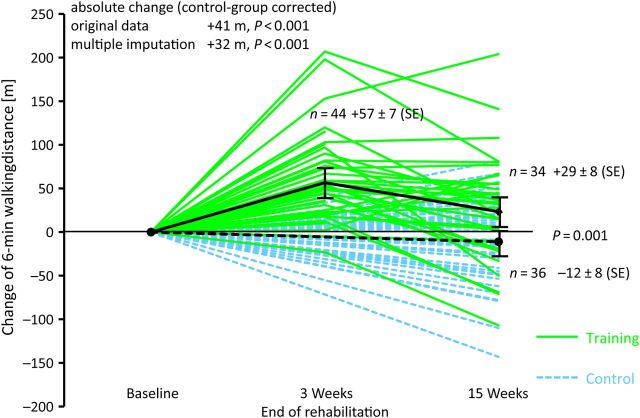
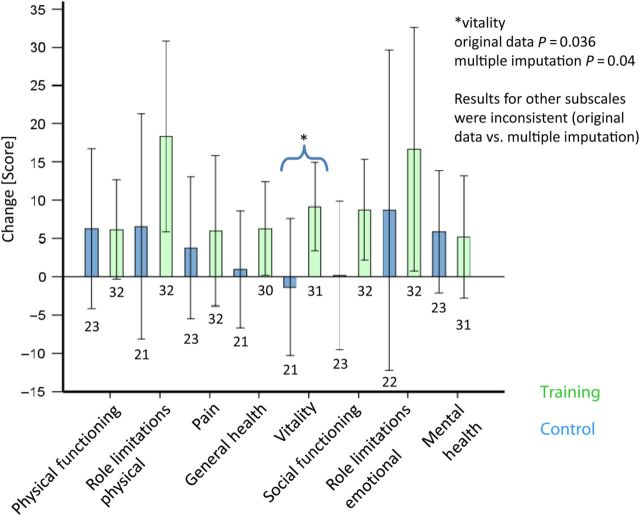
Methods and results: Eighty-seven patients with pulmonary arterial hypertension and inoperable chronic thrombo-embolic PH (54% female, 56 ± 15 years, 84% World Health Organization functional class III/IV, 53% combination therapy) on stable disease-targeted medication were randomly assigned to a control and training group. Medication remained unchanged during the study period. Non-invasive assessments and right heart catheterization at rest and during exercise were performed at baseline and after 15 weeks. Primary endpoint was the change in peak VO2/kg. Secondary endpoints included changes in haemodynamics. For missing data, multiple imputation and responder analyses were performed. The study results showed a significant improvement of peak VO2/kg in the training group (difference from baseline to 15 weeks: training +3.1 ± 2.7 mL/min/kg equals +24.3% vs. control -0.2 ± 2.3 mL/min/kg equals +0.9%, P < 0.001). Cardiac index (CI) at rest and during exercise, mean pulmonary arterial pressure, pulmonary vascular resistance, 6 min walking distance, quality of life, and exercise capacity significantly improved by exercise training.
Conclusion: Low-dose exercise training at 4-7 days/week significantly improved peak VO2/kg, haemodynamics, and further clinically relevant parameters. The improvements of CI at rest and during exercise indicate that exercise training may improve the right ventricular function. Further, large multicentre trials are necessary to confirm these results.
Keywords: Cardiac index; Cardiac output; Cardiac rehabilitation; Pulmonary hypertension; Right heart catheterization.
© The Author 2015. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Comment in
-
Exercise training in pulmonary hypertension: improving performance but waiting for outcome.Eur Heart J. 2016 Jan 1;37(1):45-8. doi: 10.1093/eurheartj/ehv440. Epub 2015 Aug 27. Eur Heart J. 2016. PMID: 26319935 No abstract available.
References
-
- Mereles D, Ehlken N, Kreuscher S, Ghofrani S, Hoeper MM, Halank M, Meyer FJ, Karger G, Buss J, Juenger J, Holzapfel N, Opitz C, Winkler J, Herth FF, Wilkens H, Katus HA, Olschewski H, Grunig E. Exercise and respiratory training improve exercise capacity and quality of life in patients with severe chronic pulmonary hypertension. Circulation 2006;114:1482–1489. - PubMed
-
- de Man FS, Handoko ML, Groepenhoff H, van 't Hul AJ, Abbink J, Koppers RJ, Grotjohan HP, Twisk JW, Bogaard HJ, Boonstra A, Postmus PE, Westerhof N, van der Laarse WJ, Vonk-Noordegraaf A. Effects of exercise training in patients with idiopathic pulmonary arterial hypertension. Eur Respir J 2009;34:669–675. - PubMed
-
- Fox BD, Kassirer M, Weiss I, Raviv Y, Peled N, Shitrit D, Kramer MR. Ambulatory rehabilitation improves exercise capacity in patients with pulmonary hypertension. J Card Fail 2011;17:196–200. - PubMed
-
- Grünig E, Lichtblau M, Ehlken N, Ghofrani HA, Reichenberger F, Staehler G, Halank M, Fischer C, Seyfarth HJ, Klose H, Meyer A, Sorichter S, Wilkens H, Rosenkranz S, Opitz C, Leuchte H, Karger G, Speich R, Nagel C. Safety and efficacy of exercise training in various forms of pulmonary hypertension. Eur Respir J 2012;40:84–92. - PubMed
-
- Chan L, Chin LM, Kennedy M, Woolstenhulme JG, Nathan SD, Weinstein AA, Connors G, Weir NA, Drinkard B, Lamberti J, Keyser RE. Benefits of intensive treadmill exercise training on cardiorespiratory function and quality of life in patients with pulmonary hypertension. Chest 2013;143:333–343. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
