

Long term outcomes of transplantation using kidneys from expanded criteria donors: prospective, population based cohort study
- PMID: 26232393
- PMCID: PMC4521904
- DOI: 10.1136/bmj.h3557
Long term outcomes of transplantation using kidneys from expanded criteria donors: prospective, population based cohort study
Abstract
Objectives: To assess the long term outcomes of transplantation using expanded criteria donors (ECD; donors aged ≥ 60 years or aged 50-59 years with vascular comorbidities) and assess the main determinants of its prognosis.
Design: Prospective, population based cohort study.
Setting: Four French referral centres.
Participants: Consecutive patients who underwent kidney transplantation between January 2004 and January 2011, and were followed up to May 2014. A validation cohort included patients from another four referral centres in France who underwent kidney transplantation between January 2002 and December 2011.
Main outcome measures: Long term kidney allograft survival, based on systematic assessment of donor, recipient, and transplant clinical characteristics; preimplantation biopsy; and circulating levels of donor specific anti-HLA (human leucocyte antigen) antibody (DSA) at baseline.
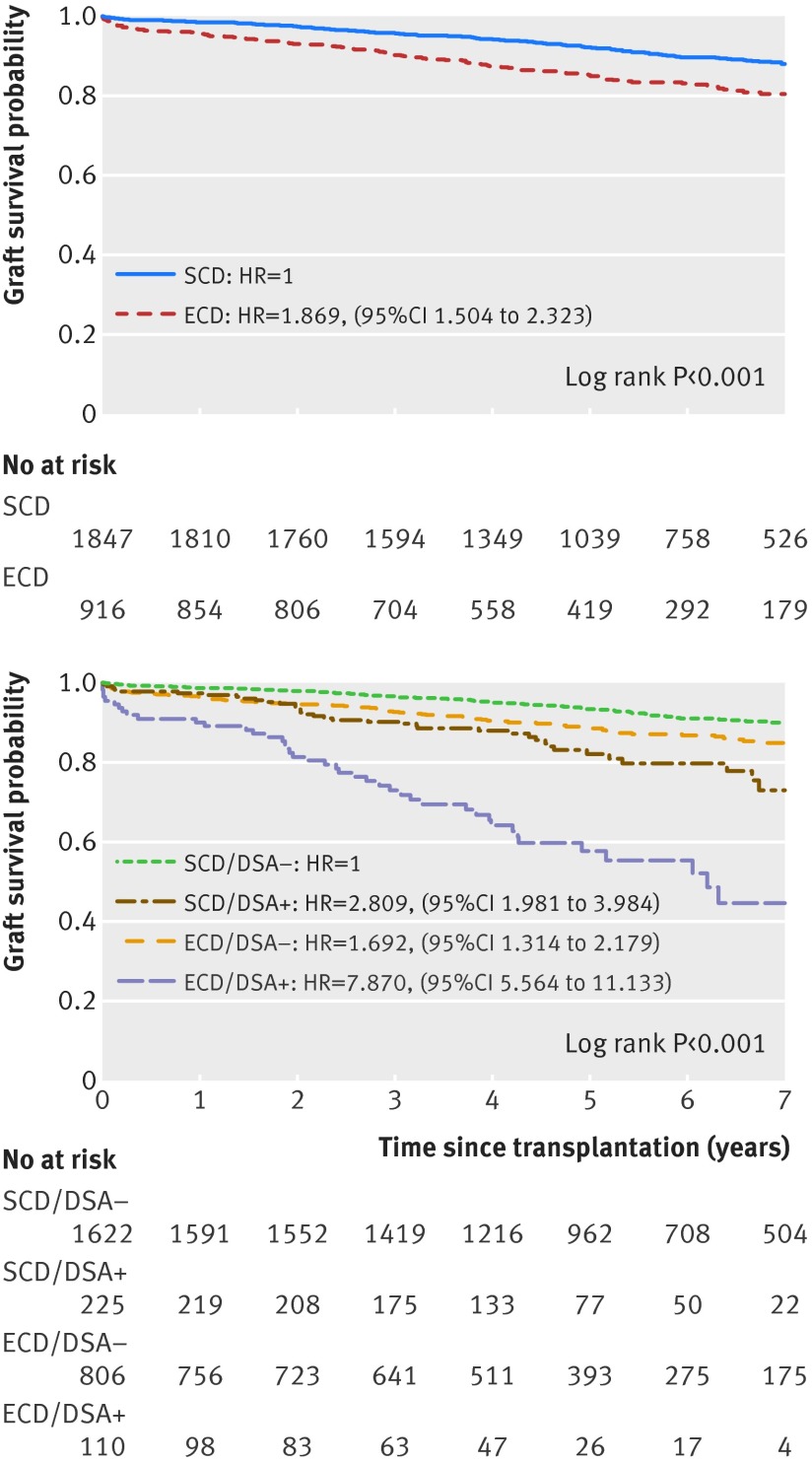
Results: The study included 6891 patients (2763 in the principal cohort, 4128 in the validation cohort). Of 2763 transplantations performed, 916 (33.2%) used ECD kidneys. Overall, patients receiving ECD transplants had lower allograft survival after seven years than patients receiving transplants from standard criteria donors (SCD; 80% v 88%, P<0.001). Patients receiving ECD transplants who presented with circulating DSA at the time of transplantation had worse allograft survival after seven years than patients receiving ECD kidneys without circulating DSA at transplantation (44% v 85%, P < 0.001). After adjusting for donor, recipient, and transplant characteristics, as well as preimplantation biopsy findings and baseline immunological parameters, the main independent determinants of long term allograft loss were identified as allocation of ECDs (hazard ratio 1.84 (95% confidence interval 1.5 to 2.3); P < 0.001), presence of circulating DSA on the day of transplantation (3.00 (2.3 to 3.9); P < 0.001), and longer cold ischaemia time (> 12 h; 1.53 (1.1 to 2.1); P = 0.011). Recipients of ECD kidneys with circulating DSA showed a 5.6-fold increased risk of graft loss compared with all other transplant therapies (P < 0.001). ECD allograft survival at seven years significantly improved with screening and transplantation in the absence of circulating DSA (P < 0.001) and with shorter (<12 h) cold ischaemia time (P=0.030), respectively. This strategy achieved ECD graft survival comparable to that of patients receiving an SCD transplant overall, translating to a 544.6 allograft life years saved during the nine years of study inclusion time.
Conclusions: Circulating DSA and cold ischaemia time are the main independent determinants of outcome from ECD transplantation. Allocation policies to avoid DSA and reduction of cold ischaemia time to increase efficacy could promote wider implement of ECD transplantation in the context of organ shortage and improve its prognosis.
© Aubert et al 2015.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Marginal kidneys for transplantation.BMJ. 2015 Aug 3;351:h3856. doi: 10.1136/bmj.h3856. BMJ. 2015. PMID: 26239226 No abstract available.
-
Transplantation: Optimizing ECD graft outcomes.Nat Rev Nephrol. 2015 Oct;11(10):567. doi: 10.1038/nrneph.2015.143. Epub 2015 Aug 18. Nat Rev Nephrol. 2015. PMID: 26281894 No abstract available.
References
-
- Réseau Epidémiologie et Information en Néphrologie. Annual report. 2013. www.socnephrologie.org/PDF/enephro/registres/rapport_2013/rapport_rein20....
-
- Evans RW, Manninen DL, Garrison LP Jr, et al. The quality of life of patients with end-stage renal disease. N Engl J Med 1985;312:553-9. - PubMed
-
- Port FK, Wolfe RA, Mauger EA, et al. Comparison of survival probabilities for dialysis patients vs cadaveric renal transplant recipients. JAMA 1993;270:1339-43. - PubMed
-
- Rana A, Gruessner A, Agopian VG, et al. Survival benefit of solid-organ transplant in the United States. JAMA Surg 2015;150:252-9. - PubMed
-
- Port FK, Bragg-Gresham JL, Metzger RA, et al. Donor characteristics associated with reduced graft survival: an approach to expanding the pool of kidney donors. Transplantation 2002;74:1281-6. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials