

Development of Prototype Filovirus Recombinant Antigen Immunoassays
- PMID: 26232440
- PMCID: PMC4564556
- DOI: 10.1093/infdis/jiv353
Development of Prototype Filovirus Recombinant Antigen Immunoassays
Abstract
Background: Throughout the 2014-2015 Ebola outbreak in West Africa, major gaps were exposed in the availability of validated rapid diagnostic platforms, protective vaccines, and effective therapeutic agents. These gaps potentiated the development of prototype rapid lateral flow immunodiagnostic (LFI) assays that are true point-of-contact platforms, for the detection of active Ebola infections in small blood samples.
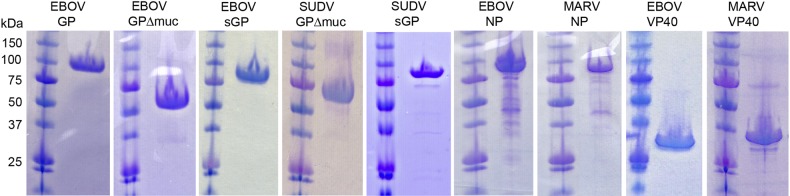
Methods: Recombinant Ebola and Marburg virus matrix VP40 and glycoprotein (GP) antigens were used to derive a panel of monoclonal and polyclonal antibodies. Antibodies were tested using a multivariate approach to identify antibody-antigen combinations suitable for enzyme-linked immunosorbent assay (ELISA) and LFI assay development.
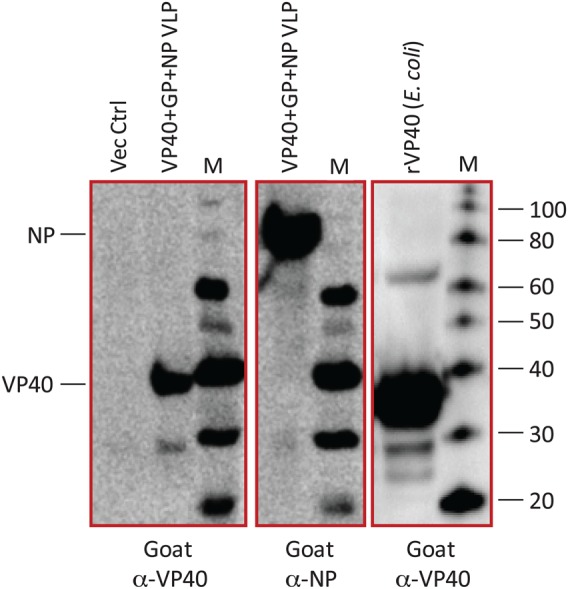
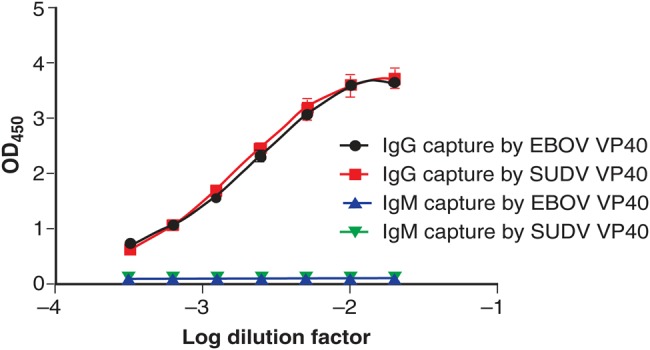
Results: Polyclonal antibodies generated in goats were superior reagents for capture and detection of recombinant VP40 in test sample matrices. These antibodies were optimized for use in antigen-capture ELISA and LFI assay platforms. Prototype immunoglobulin M (IgM)/immunoglobulin G (IgG) ELISAs were similarly developed that specifically detect Ebola virus-specific antibodies in the serum of experimentally infected nonhuman primates and in blood samples obtained from patients with Ebola from Sierra Leone.
Conclusions: The prototype recombinant Ebola LFI assays developed in these studies have sensitivities that are useful for clinical diagnosis of acute ebolavirus infections. The antigen-capture and IgM/IgG ELISAs provide additional confirmatory assay platforms for detecting VP40 and other ebolavirus-specific immunoglobulins.
Keywords: ELISA; Ebola; Ebola virus; filovirus; lateral flow immunodiagnostic; point-of-care testing.
© The Author 2015. Published by Oxford University Press on behalf of the Infectious Diseases Society of America. All rights reserved. For Permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Centers for Disease Control and Prevention. Ebola outbreaks 2000–2014. http://www.cdc.gov/vhf/ebola/resources/outbreaks.html. Accessed 8 April 2015.
-
- Kortepeter MG, Smith PW, Hewlett A, Cieslak TJ. Caring for patients with Ebola: a challenge in any care facility. Ann Intern Med 2015; 162:68–9. - PubMed
-
- Fowler RA, Fletcher T, Fischer WA II et al. . Caring for critically ill patients with Ebola virus disease. Perspectives from West Africa. Am J Respir Crit Care Med 2014; 190:733–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U01 AI082119/AI/NIAID NIH HHS/United States
- AI081982/AI/NIAID NIH HHS/United States
- AI104621/AI/NIAID NIH HHS/United States
- R01 AI081982/AI/NIAID NIH HHS/United States
- AI115754/AI/NIAID NIH HHS/United States
- AI082119/AI/NIAID NIH HHS/United States
- AI067927/AI/NIAID NIH HHS/United States
- R13 AI104216/AI/NIAID NIH HHS/United States
- R01 AI067927/AI/NIAID NIH HHS/United States
- R44 AI115754/AI/NIAID NIH HHS/United States
- AI104216/AI/NIAID NIH HHS/United States
- AI067188/AI/NIAID NIH HHS/United States
- U19 AI109762/AI/NIAID NIH HHS/United States
- U01 AI070530/AI/NIAID NIH HHS/United States
- AI088843/AI/NIAID NIH HHS/United States
- HHSN272200900049C/AI/NIAID NIH HHS/United States
- R44 AI088843/AI/NIAID NIH HHS/United States
- AI070530/AI/NIAID NIH HHS/United States
- R01 AI104621/AI/NIAID NIH HHS/United States
- UC1 AI067188/AI/NIAID NIH HHS/United States
- AI082805/AI/NIAID NIH HHS/United States
- R43 AI088843/AI/NIAID NIH HHS/United States
- HHSN272200900049C/PHS HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
