

Identifying the Optimal Role for Pharmacists in Care Transitions: A Systematic Review
- PMID: 26233535
- PMCID: PMC10397897
- DOI: 10.18553/jmcp.2015.21.8.614
Identifying the Optimal Role for Pharmacists in Care Transitions: A Systematic Review
Abstract
Background: A transition from one health care setting to another increases the risk of medication errors. Several strategies have been applied to improve care transitions and reduce adverse clinical outcomes. Pharmacist intervention during and after hospitalization has been frequently studied and show a variable effect on these outcomes.
Objective: To identify the components of pharmacist intervention that improve clinical outcomes during care transitions.
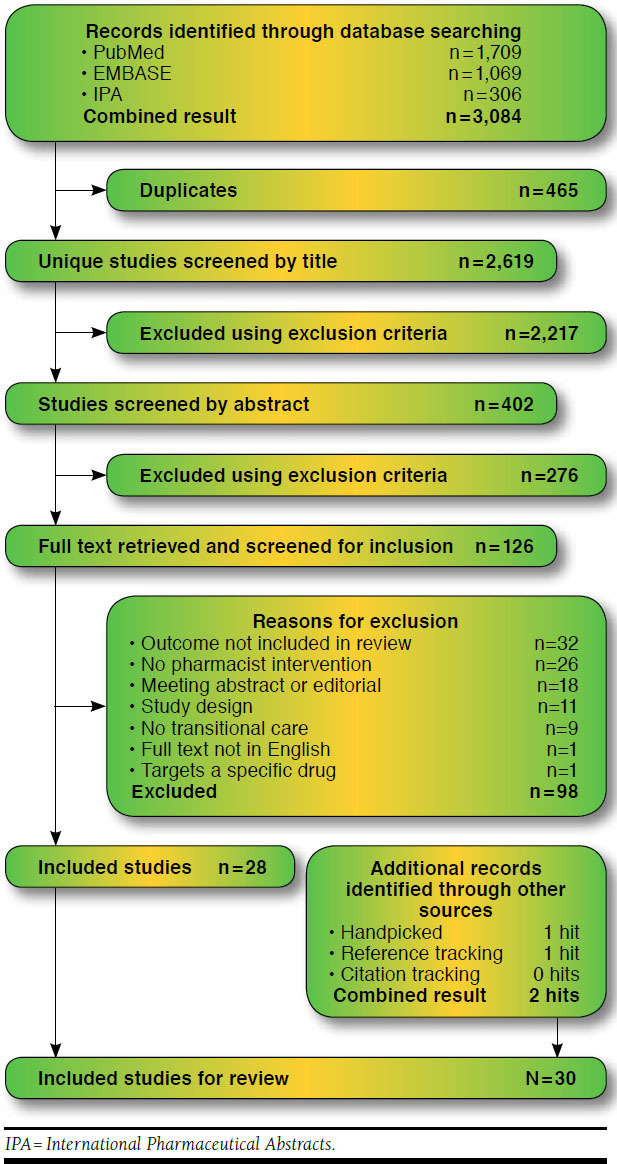
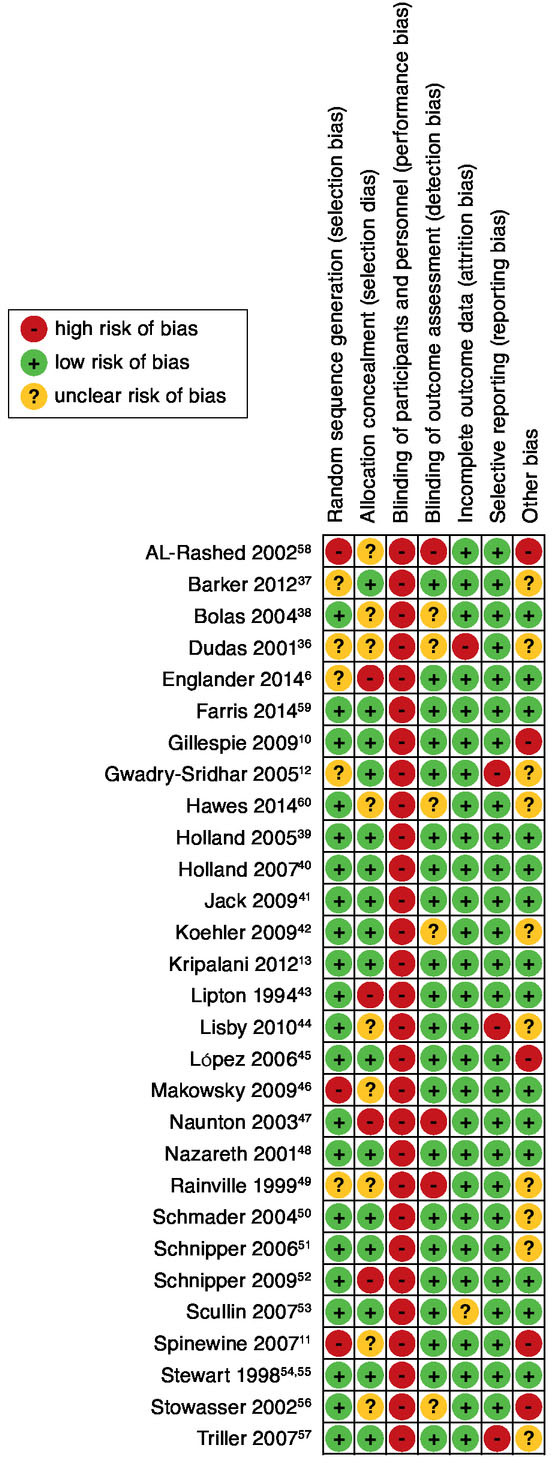
Methods: MEDLINE, EMBASE, International Pharmaceutical Abstracts, and Web of Science databases were searched for randomized controlled trials (RCTs) that studied pharmacist intervention with regard to hospitalization. Two reviewers independently screened all references published from inception to November 2014, extracted data, and assessed risk of bias.
Results: A total of 30 studies met the inclusion criteria. A model was created to categorize and cluster components of pharmacist intervention. The average number of components deployed, stages of hospitalization covered, and intervention targets were equally distributed between effective and ineffective studies. A best evidence synthesis of 15 studies revealed strong evidence for a clinical medication review in multifaceted programs (5 effective vs. 0 ineffective studies). Conflicting evidence was found for an isolated postdischarge intervention, admission medication reconciliation, combining postdischarge interventions with in-hospital interventions, and covering of multiple stages. Closely collaborating with other health care providers enhanced the effectiveness.
Conclusions: Although there is a need for well-designed and well-reported RCTs, the study heterogeneity enabled a best evidence synthesis to elucidate effective components of pharmacist intervention. In isolated postdischarge intervention programs, evidence tends towards collaborating with nurses and tailoring to individual patient needs. In multifaceted intervention programs, performing medication reconciliation alone is insufficient in reducing postdischarge clinical outcomes and should be combined with active patient counseling and a clinical medication review. Furthermore, close collaboration between pharmacists and physicians is beneficial. Finally, it is important to secure continuity of care by integrating pharmacists in these multifaceted programs across health care settings. Ultimately, pharmacists need to know patient clinical background and previous hospital experience.
Conflict of interest statement
No funds were received for conducting this review. The authors attest that they have no financial interests, arrangements, or other conflicts of interest to disclose.
Bouvy had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design were contributed by Ensing, Stuijt, Koster, and Bouvy. Data were collected by Ensing and Stuijt and interpretated by Ensing, Stuijt, Karapinar-Çarkit, Koster, and Bouvy. The manuscript was written by Ensing, Stuijt, Koster, and Bouvy and revised by van den Bemt, van Dooren, Karapinar-Çarkit, and Koster.
Figures
References
-
- Borgsteede SD, Karapinar-Çarkit F, Hoffmann E, Zoer J, van den Bemt PM. Information needs about medication according to patients discharged from a general hospital. Patient Educ Couns. 2011;83(1):22-28. - PubMed
-
- Witherington EM, Pirzada OM, Avery AJ. Communication gaps and readmissions to hospital for patients aged 75 years and older: observational study. Qual Saf Health Care. 2008;17(1):71-75. - PubMed
-
- Poston KM, Dumas BP, Edlund BJ. Outcomes of a quality improvement project implementing stroke discharge advocacy to reduce 30-day readmission rates. J Nurs Care Qual. 2014;29(3):237-44. - PubMed
-
- White CM. Pharmacists need recognition as providers to enhance patient care. Ann Pharmacother. 2014;48(2):268-73. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
