

Vosaroxin plus cytarabine versus placebo plus cytarabine in patients with first relapsed or refractory acute myeloid leukaemia (VALOR): a randomised, controlled, double-blind, multinational, phase 3 study
- PMID: 26234174
- PMCID: PMC4822512
- DOI: 10.1016/S1470-2045(15)00201-6
Vosaroxin plus cytarabine versus placebo plus cytarabine in patients with first relapsed or refractory acute myeloid leukaemia (VALOR): a randomised, controlled, double-blind, multinational, phase 3 study
Abstract
Background: Safe and effective treatments are urgently needed for patients with relapsed or refractory acute myeloid leukaemia. We investigated the efficacy and safety of vosaroxin, a first-in-class anticancer quinolone derivative, plus cytarabine in patients with relapsed or refractory acute myeloid leukaemia.
Methods: This phase 3, double-blind, placebo-controlled trial was undertaken at 101 international sites. Eligible patients with acute myeloid leukaemia were aged 18 years of age or older and had refractory disease or were in first relapse after one or two cycles of previous induction chemotherapy, including at least one cycle of anthracycline (or anthracenedione) plus cytarabine. Patients were randomly assigned 1:1 to vosaroxin (90 mg/m(2) intravenously on days 1 and 4 in a first cycle; 70 mg/m(2) in subsequent cycles) plus cytarabine (1 g/m(2) intravenously on days 1-5) or placebo plus cytarabine through a central interactive voice system with a permuted block procedure stratified by disease status, age, and geographical location. All participants were masked to treatment assignment. The primary efficacy endpoint was overall survival and the primary safety endpoint was 30-day and 60-day all-cause mortality. Efficacy analyses were done by intention to treat; safety analyses included all treated patients. This study is registered with ClinicalTrials.gov, number NCT01191801.
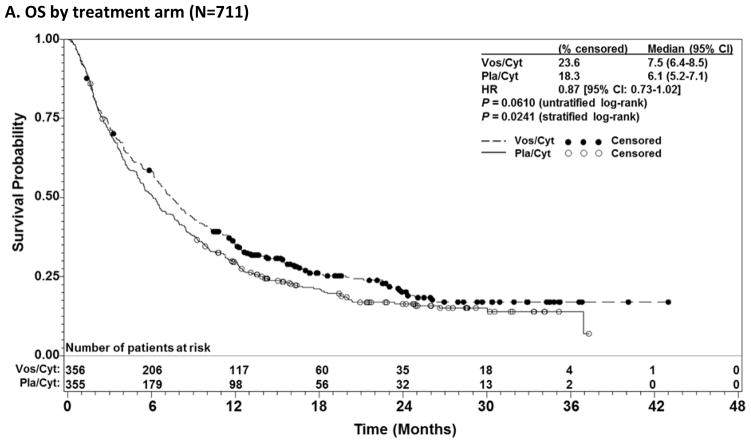
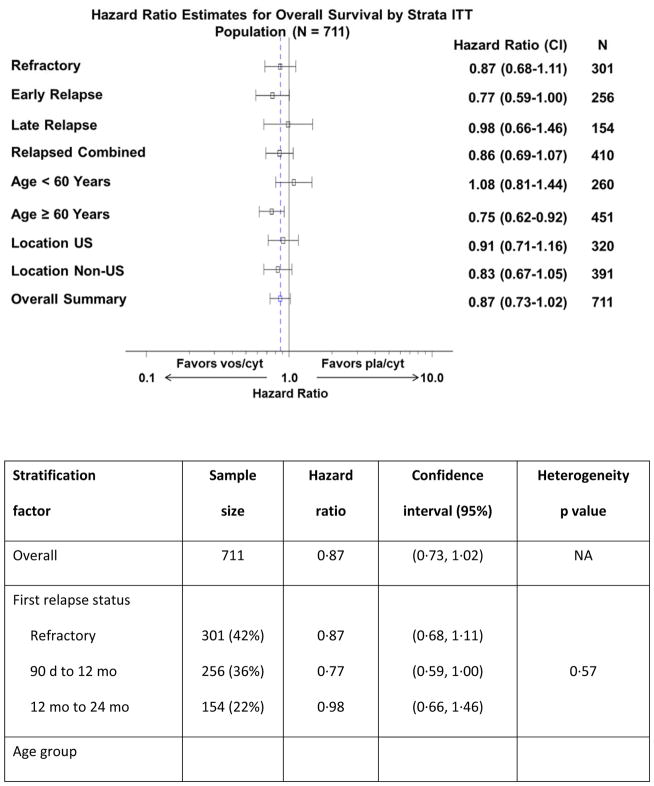
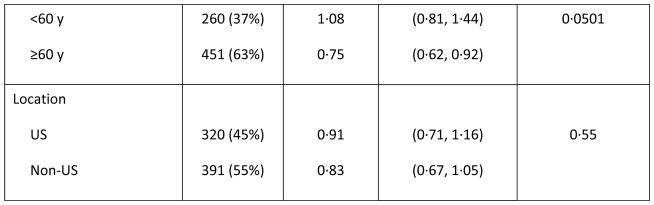
Findings: Between Dec 17, 2010, and Sept 25, 2013, 711 patients were randomly assigned to vosaroxin plus cytarabine (n=356) or placebo plus cytarabine (n=355). At the final analysis, median overall survival was 7·5 months (95% CI 6·4-8·5) in the vosaroxin plus cytarabine group and 6·1 months (5·2-7·1) in the placebo plus cytarabine group (hazard ratio 0·87, 95% CI 0·73-1·02; unstratified log-rank p=0·061; stratified p=0·024). A higher proportion of patients achieved complete remission in the vosaroxin plus cytarabine group than in the placebo plus cytarabine group (107 [30%] of 356 patients vs 58 [16%] of 355 patients, p<0·0001). Early mortality was similar between treatment groups (30-day: 28 [8%] of 355 patients in the vosaroxin plus cytarabine group vs 23 [7%] of 350 in the placebo plus cytarabine group; 60-day: 70 [20%] vs 68 [19%]). Treatment-related deaths occurred at any time in 20 (6%) of 355 patients given vosaroxin plus cytarabine and in eight (2%) of 350 patients given placebo plus cytarabine. Treatment-related serious adverse events occurred in 116 (33%) and 58 (17%) patients in each group, respectively. Grade 3 or worse adverse events that were more frequent in the vosaroxin plus cytarabine group than in the placebo plus cytarabine group included febrile neutropenia (167 [47%] vs 117 [33%]), neutropenia (66 [19%] vs 49 [14%]), stomatitis (54 [15%] vs 10 [3%]), hypokalaemia (52 [15%] vs 21 [6%]), bacteraemia (43 [12%] vs 16 [5%]), sepsis (42 [12%] vs 18 [5%]), and pneumonia (39 [11%] vs 26 [7%]).
Interpretation: Although there was no significant difference in the primary endpoint between groups, the prespecified secondary analysis stratified by randomisation factors suggests that the addition of vosaroxin to cytarabine might be of clinical benefit to some patients with relapsed or refractory acute myeloid leukaemia.
Funding: Sunesis Pharmaceuticals.
Copyright © 2015 Elsevier Ltd. All rights reserved.
Conflict of interest statement
FR reports grants and advisory fees from Sunesis during the conduct of the study, and grants from Sunesis outside the submitted work. NV reports advisory fees from Sunesis during the conduct of the study. SAS and AW report advisory fees from Sunesis outside the submitted work. HPE reports grants and consulting fees from Sunesis during the conduct of the study, and reports fees from Novartis, Incyte, Celgene, Ariad, and Seattle Genetics and grants from Millennium, Seattle Genetics, Celator, Amgen, and Astellas, outside the submitted work. CR reports advisory fees from Sunesis during the conduct of the study, and reports grants from Amgen, Chugai, and Celgene and advisory fees from Celgene outside the submitted work. VMK and GJR report clinical trial support from Sunesis during the conduct of the study and advisory fees from Sunesis outside the submitted work. JC reports grants from Ambit, Arog, Astellas, Celator, Novartis and consulting fees from Novartis and Astellas, outside the submitted work. OO reports grants from Sunesis during the conduct of the study, and reports fees from Sunesis, Algeta, and Spectrum Pharmaceuticals and grants from Astex, MEI-Pharma, Topotarget, Lilly, and Celgene outside the submitted work. MH reports grants and consulting fees from Sunesis during the conduct of the study. LD reports research funds from Sunesis during the conduct of the study, and reports consulting fees from Maxygen and research funds from Celator outside the submitted work. GG reports fees from Amgen, Celgene, GlaxoSmithKline, Janssen, Novartis, and Roche, outside the submitted work. RKS reports grants and advisory fees from Sunesis during the conduct of the study. CM is an employee of Cytel Inc. and receives no remuneration other than his Cytel salary; he has nothing to disclose. ARC, JAF, RW, JAS, and GA were employed by Sunesis Pharmaceuticals during the conduct of the study. EKR, HS, JEL, MEC, GJS, EJ, AP, H-AH, XT, VH, JM, H-GD, BLP, A-MC, and DH have nothing to disclose.
Figures
Comment in
-
Vosaroxin in acute myeloid leukaemia.Lancet Oncol. 2015 Sep;16(9):1000-1001. doi: 10.1016/S1470-2045(15)00165-5. Epub 2015 Jul 30. Lancet Oncol. 2015. PMID: 26234173 No abstract available.
References
-
- Breems DA, Van Putten WL, Huijgens PC, et al. Prognostic index for adult patients with acute myeloid leukemia in first relapse. J Clin Oncol. 2005;23:1969–78. - PubMed
-
- National Comprehensive Cancer Network. [accessed April 6, 2015];NCCN Clinical Practice Guidelines in Oncology: acute myeloid leukemia. Version 1.2015. http://www.nccn.org/professionals/physician_gls/pdf/aml.pdf.
-
- Roboz GJ, Rosenblat T, Arellano M, et al. International randomized phase III study of elacytarabine versus investigator choice in patients with relapsed/refractory acute myeloid leukemia. J Clin Oncol. 2014;32:1919–26. - PubMed
-
- Ferrara F, Palmieri S, Mele G. Prognostic factors and therapeutic options for relapsed or refractory acute myeloid leukemia. Haematologica. 2004;89:998–1008. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
