

Use of Methyl Tert-Butyl Ether for the Treatment of Refractory Intrahepatic Biliary Strictures and Bile Casts: A Modern Perspective
- PMID: 26236535
- PMCID: PMC4508463
- DOI: 10.1155/2015/408175
Use of Methyl Tert-Butyl Ether for the Treatment of Refractory Intrahepatic Biliary Strictures and Bile Casts: A Modern Perspective
Abstract
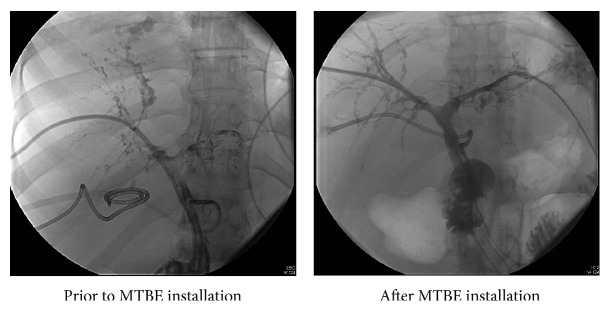
Cholelithiasis is a prevalent problem in the United States with 14% or more adults affected. Definitive treatment of cholelithiasis is cholecystectomy. When cholecystectomy yields minimal resolution treatment options include expectant management of asymptomatic gallstones or endoscopic retrograde cholangiopancreatogram. We present a case of intrahepatic biliary casts where surgical option was not possible, interventional radiology was unsuccessful, and methyl tert-butyl ether was used to dissolve the biliary obstruction. Dissolution therapy of gallstones was first reported in 1722 when Vollisnieri used turpentine in vitro. While diethyl ether has excellent solubilizing capacity, its low boiling point limited its use surgically as it vaporizes immediately. Diethyl ether can expand 120-fold during warming to body temperature after injection into the biliary system making it impractical for routine use. The use of dissolution is out of favor due to the success of laparoscopic cholecystectomy. Epidemiological studies have shown the general population should have minimal concerns from passive exposure. Dissolution using MTBE remains a viable option if surgical or endoscopic options are not available. However, because of risks involved to both the patient and the staff, careful multidisciplinary team approach must be undertaken to minimize the risks and provide the best possible care to the patient.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
