

A case of pulmonary lymphangioleiomyomatosis complicated with uterine and retroperitoneal tumors
- PMID: 26236608
- PMCID: PMC4501452
- DOI: 10.1016/j.rmcr.2015.02.001
A case of pulmonary lymphangioleiomyomatosis complicated with uterine and retroperitoneal tumors
Abstract
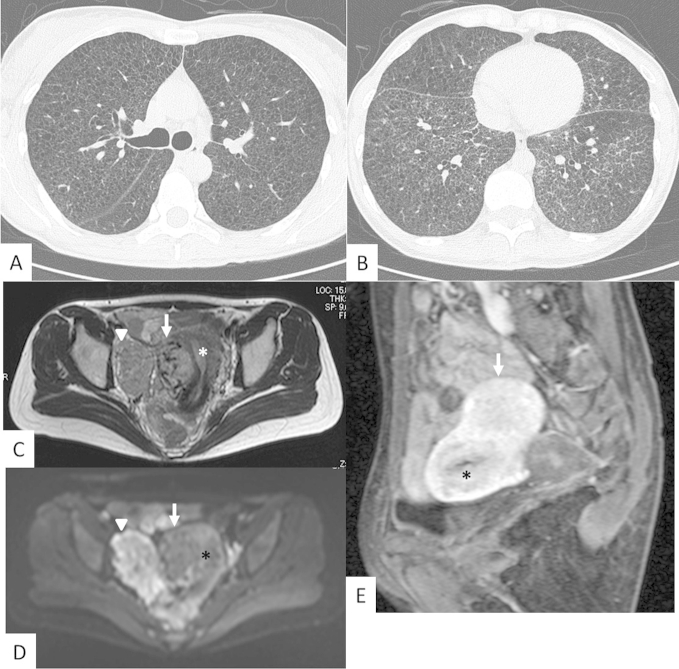
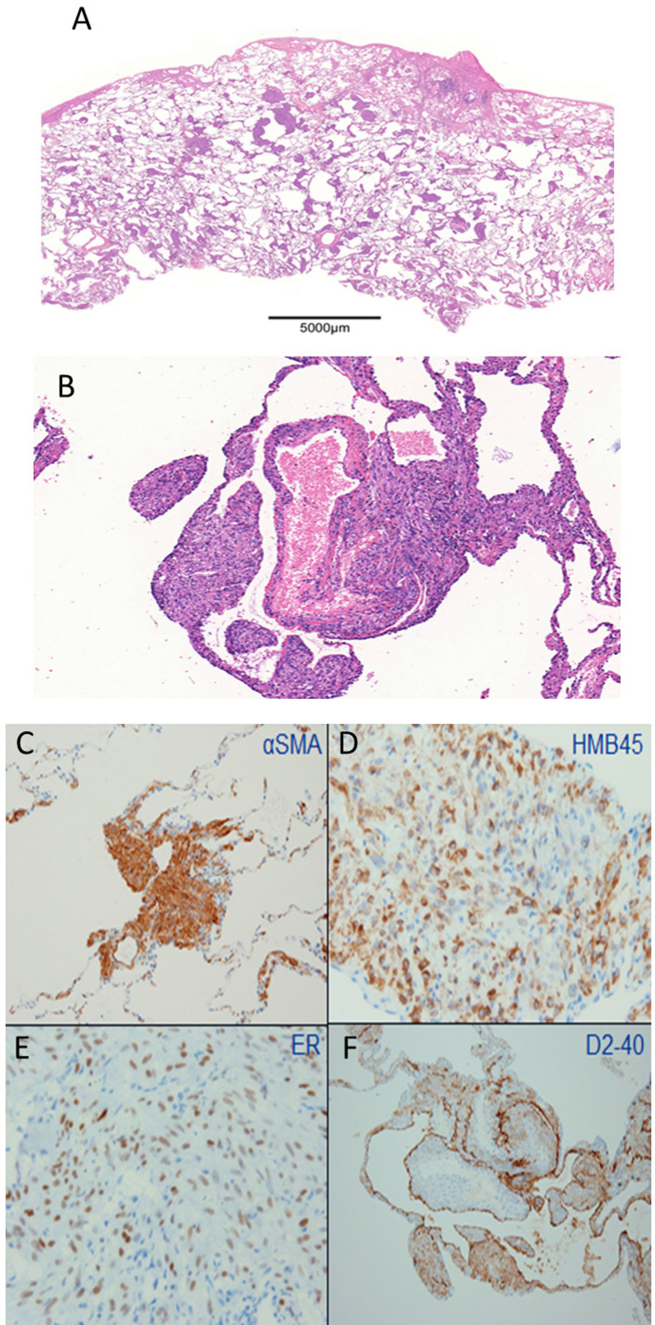
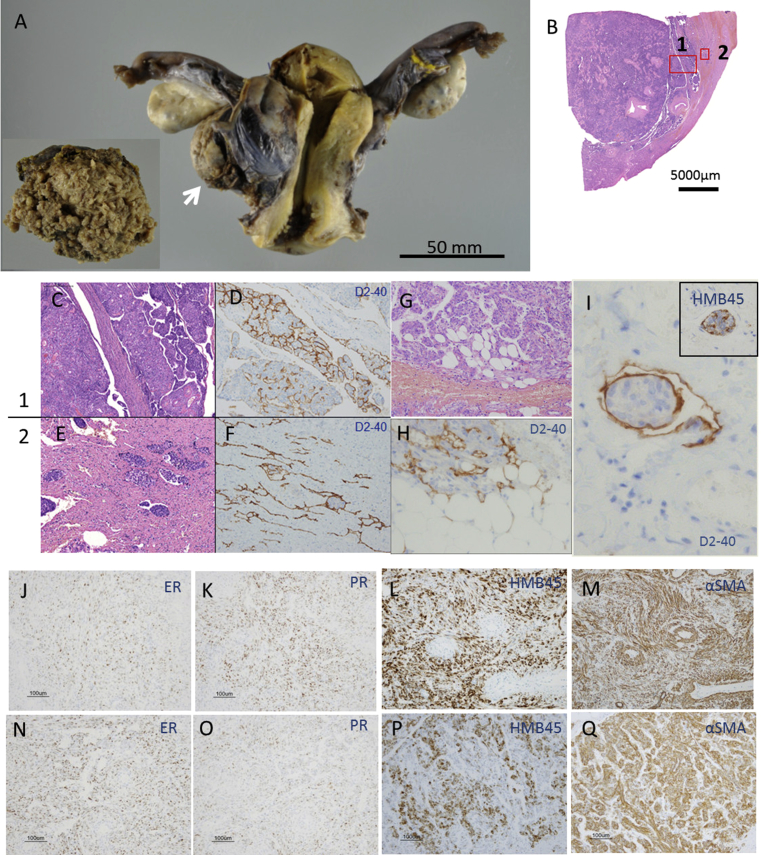
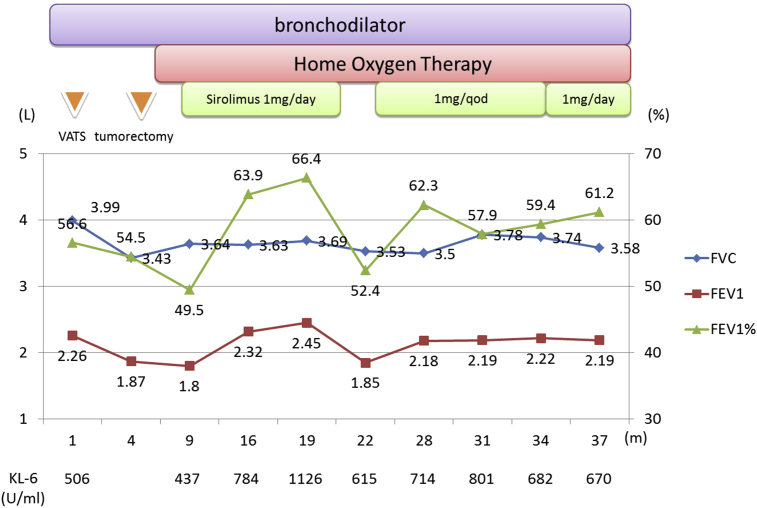
A 39-year-old female experienced dyspnea on exertion for eight months. Chest CT demonstrated findings of Lymphangioleiomyomatosis (LAM), including diffuse thin-walled cystic lesions. A surgical lung biopsy revealed human melanoma black-45-positive cell infiltration and aggregation, resulting in a diagnosis of sporadic LAM without tuberous sclerosis complex. Pelvic MRI showed two large tumors, one of which was in the myometrium and the other was in the retroperitoneal space. Because we were not able to exclude the presence of malignant tumors using MR imaging, the tumors were surgically resected. The histopathology demonstrated the resected tumors to be composed of LAM cells. The patient's symptoms worsened, and sirolimus was administered, which improved the dyspnea and pulmonary function. The adverse effect was mild liver damage. Following the initiation of treatment with sirolimus, transient elevation of the serum KL-6 level was detected without interstitial pneumonia. This LAM case complicated with large uterine and retroperitoneal tumors was successfully treated with surgical resection and sirolimus.
Keywords: KL-6; Lymphangioleiomyomatosis; Retroperitoneal tumor; Sirolimus; Uterine tumor.
Figures
Similar articles
-
Pulmonary lymphangioleiomyomatosis in a 46-year-old female: A case report and review of the literature.Biomed Rep. 2016 Jun;4(6):719-722. doi: 10.3892/br.2016.652. Epub 2016 Apr 13. Biomed Rep. 2016. PMID: 27284412 Free PMC article.
-
Therapeutic Effect of Sirolimus for Lymphangioleiomyomatosis Remaining in the Abdominopelvic Region After Lung Transplantation: A Case Report.Transplant Proc. 2016 Jan-Feb;48(1):271-4. doi: 10.1016/j.transproceed.2015.12.021. Transplant Proc. 2016. PMID: 26915883
-
Incidental Pelvic and Para-aortic Lymph Node Lymphangioleiomyomatosis Detected During Surgical Staging of Pelvic Cancer in Women Without Symptomatic Pulmonary Lymphangioleiomyomatosis or Tuberous Sclerosis Complex.Am J Surg Pathol. 2015 Aug;39(8):1015-25. doi: 10.1097/PAS.0000000000000416. Am J Surg Pathol. 2015. PMID: 25786086
-
[Treatment of pulmonary and retroperitoneal lymphangioleiomyomatosis with rapamycin: a case presentation and literature review].Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2012 Sep;37(9):963-7. doi: 10.3969/j.issn.1672-7347.2012.09.019. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2012. PMID: 23000776 Review. Chinese.
-
Extrapulmonary lymphangioleiomyomatosis and lymphangiomatous cysts in tuberous sclerosis complex.Mayo Clin Proc. 1995 Jul;70(7):641-8. doi: 10.4065/70.7.641. Mayo Clin Proc. 1995. PMID: 7791386 Review.
Cited by
-
Pulmonary lymphangioleiomyomatosis in a 46-year-old female: A case report and review of the literature.Biomed Rep. 2016 Jun;4(6):719-722. doi: 10.3892/br.2016.652. Epub 2016 Apr 13. Biomed Rep. 2016. PMID: 27284412 Free PMC article.
-
Low-dose sirolimus in retroperitoneal lymphangioleiomyomas.Lung India. 2019 Jul-Aug;36(4):349-352. doi: 10.4103/lungindia.lungindia_433_18. Lung India. 2019. PMID: 31290423 Free PMC article.
-
Extrapulmonary uterine lymphangioleiomyomatosis (LAM) and dysfunctional uterine bleeding: the first presentation of LAM in a tuberous sclerosis complex patient.BMJ Case Rep. 2019 Feb 25;12(2):e226358. doi: 10.1136/bcr-2018-226358. BMJ Case Rep. 2019. PMID: 30804158 Free PMC article.
References
-
- Carrington C.B., Cugell D.W., Gaensler E.A., Marks A., Redding R.A., Schaaf J.T. Lymphangioleiomyomatosis: physiologic-pathologic-radiologic correlations. Am. Rev. Respir. Dis. 1977;116:977–995. - PubMed
-
- Bernstein S.M., Newell J.D., Jr., Adamczyk D., Mortenson R.L., King T.E., Jr., Lynch D.A. How common are renal angiomyolipomas in patients with pulmonary lymphangiomyomatosis? Am. J. Respir. Crit. Care Med. 1995;152:2138–2143. - PubMed
-
- Hohman D.W., Noghrehkar D., Ratnayake S. Lymphangioleiomyomatosis: a review. Eur. J. Intern Med. 2008;19:319–324. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
