

Vasopressors for the Treatment of Septic Shock: Systematic Review and Meta-Analysis
- PMID: 26237037
- PMCID: PMC4523170
- DOI: 10.1371/journal.pone.0129305
Vasopressors for the Treatment of Septic Shock: Systematic Review and Meta-Analysis
Abstract
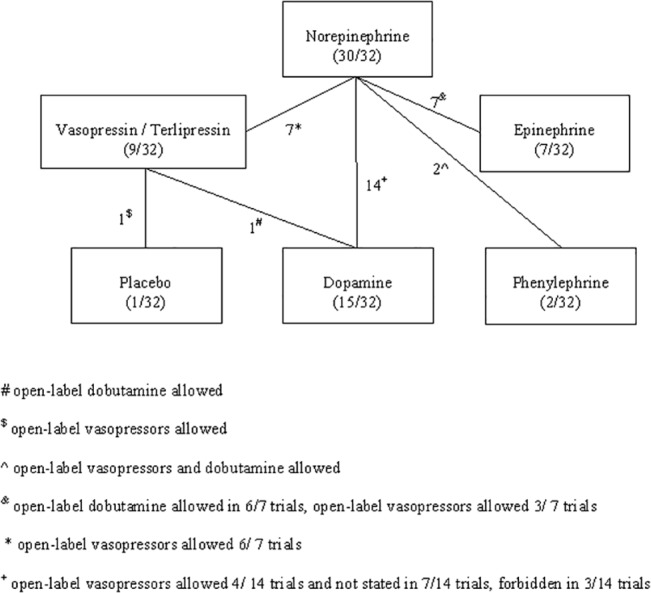
Objective: International guidelines recommend dopamine or norepinephrine as first-line vasopressor agents in septic shock. Phenylephrine, epinephrine, vasopressin and terlipressin are considered second-line agents. Our objective was to assess the evidence for the efficiency and safety of all vasopressors in septic shock.
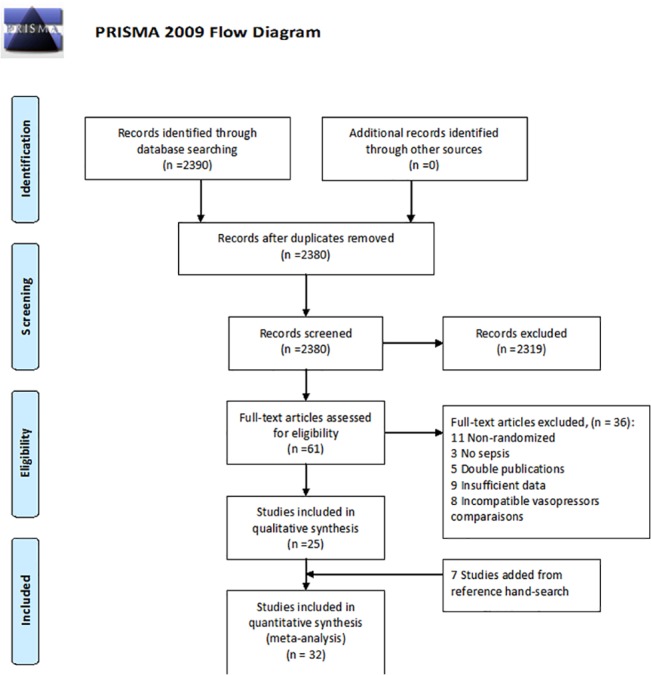
Methods: Systematic review and meta-analysis. We searched electronic database of MEDLINE, CENTRAL, LILACS and conference proceedings up to June 2014. We included randomized controlled trials comparing different vasopressors for the treatment of adult patients with septic shock. Primary outcome was all-cause mortality. Other clinical and hemodynamic measurements were extracted as secondary outcomes. Risk ratios (RR) and mean differences with 95% confidence intervals (CI) were pooled.
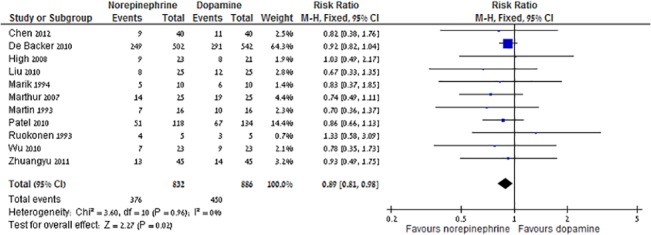
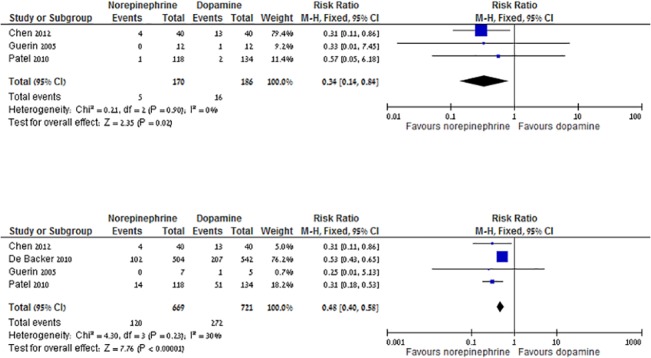
Results: Thirty-two trials (3,544 patients) were included. Compared to dopamine (866 patients, 450 events), norepinephrine (832 patients, 376 events) was associated with decreased all-cause mortality, RR 0.89 (95% CI 0.81-0.98), corresponding to an absolute risk reduction of 11% and number needed to treat of 9. Norepinephrine was associated with lower risk for major adverse events and cardiac arrhythmias compared to dopamine. No other mortality benefit was demonstrated for the comparisons of norepinephrine to epinephrine, phenylephrine and vasopressin / terlipressin. Hemodynamic data were similar between the different vasopressors, with some advantage for norepinephrine in central venous pressure, urinary output and blood lactate levels.
Conclusions: Evidence suggests a survival benefit, better hemodynamic profile and reduced adverse events rate for norepinephrine over dopamine. Norepinephrine should be regarded as the first line vasopressor in the treatment of septic shock.
Conflict of interest statement
Figures
References
-
- Annane D, Aegerter P, Jars-Guincestre MC, Guidet B (2003) Current epidemiology of septic shock: the CUB-Rea Network. Am J Respir Crit Care Med 168: 165–172. - PubMed
-
- Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR (2001) Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med 29: 1303–1310. - PubMed
-
- Friedman G, Silva E, Vincent JL (1998) Has the mortality of septic shock changed with time. Crit Care Med 26: 2078–2086. - PubMed
-
- (1992) American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference: definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Crit Care Med 20: 864–874. - PubMed
-
- Rivers E, Nguyen B, Havstad S, Ressler J, Muzzin A, Knobilch B et al. (2001) Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med 345: 1368–1377. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
