

Masquerading optic neuritis
- PMID: 26240099
- PMCID: PMC4533613
- DOI: 10.1136/bcr-2015-210259
Masquerading optic neuritis
Abstract
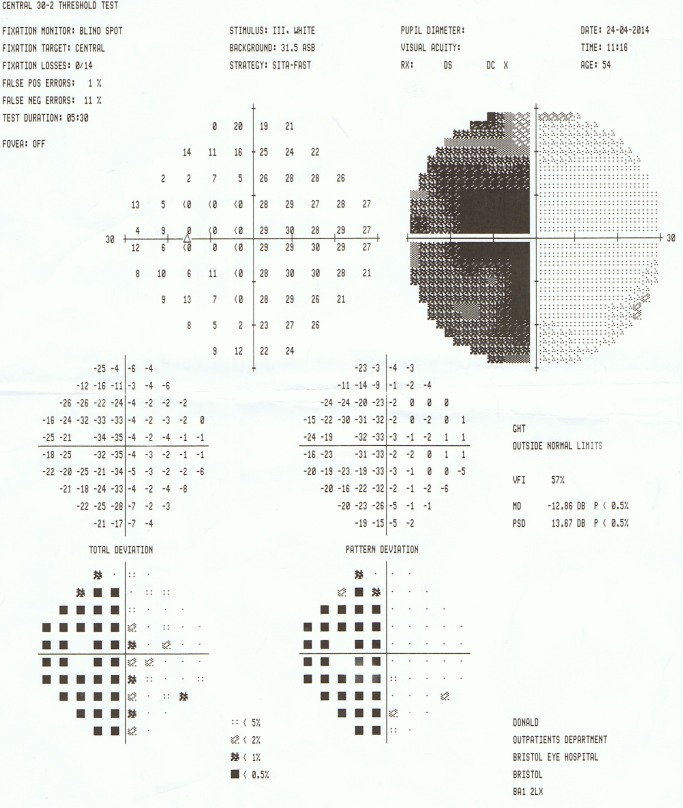
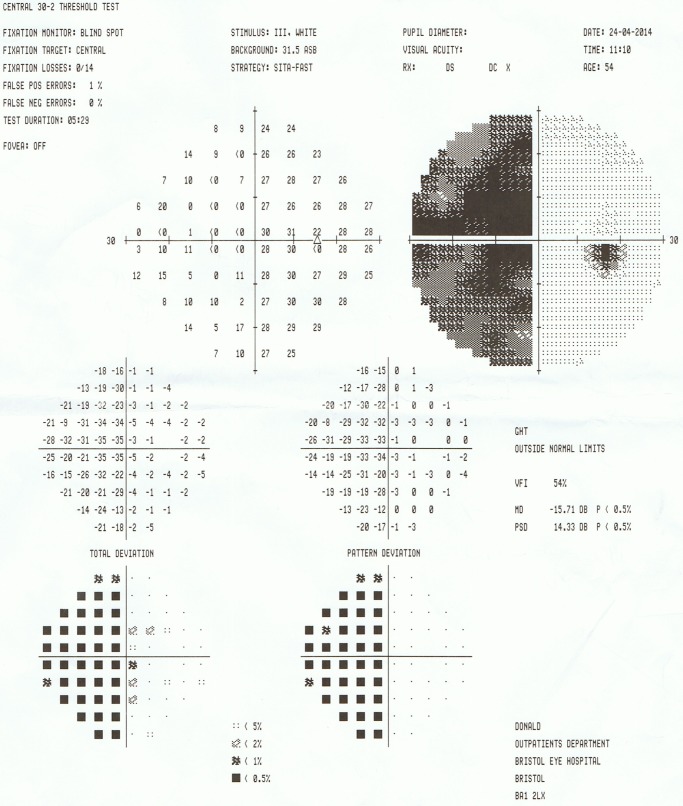
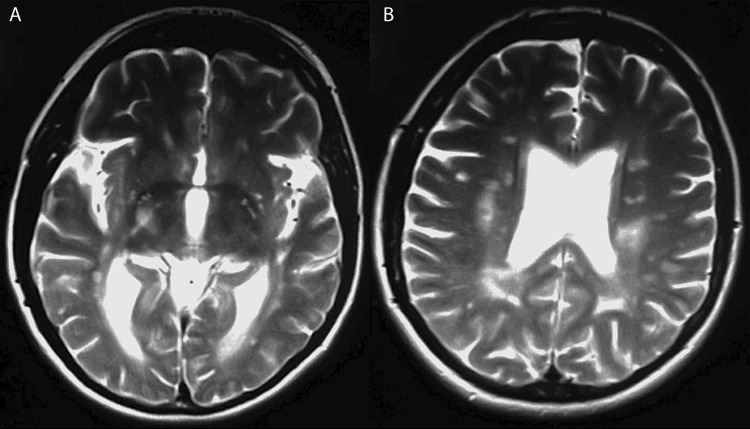
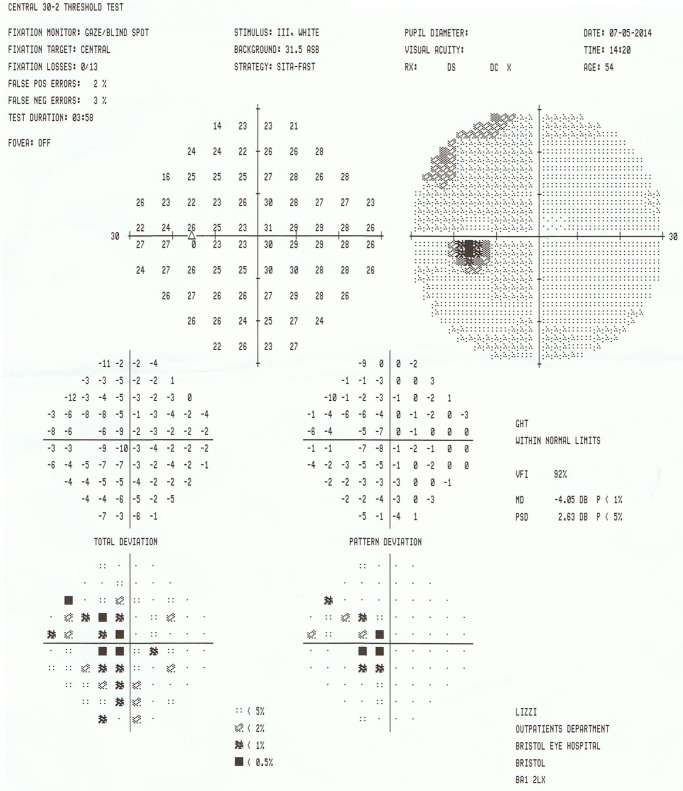
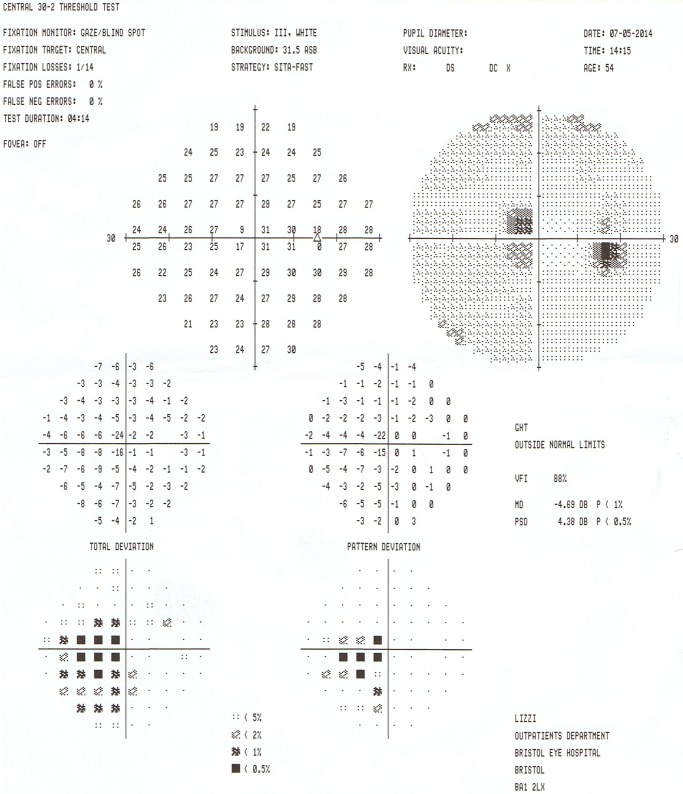
A 54-year-old woman presented to the ophthalmology emergency department with a 10-day history of blurred vision. The best-corrected visual acuities and Ishihara colour vision were bilaterally reduced with a left relative afferent pupillary defect. Slit-lamp examination was otherwise normal. Retrobulbar optic neuritis (ON) was presumed as she had suffered with this previously and was known to have multiple sclerosis (MS). She was recalled the following week for visual field (VF) testing, which was not available at the time of presentation. VFs demonstrated an incongruous left homonymous hemianopia. She was immediately referred to the medical team to investigate for a stroke, which was subsequently excluded. Thereafter, a trial of pulsed methylprednisolone was commenced, resulting in near complete resolution of the hemianopia. This case demonstrates not only the importance of VF testing, but also how ON may present with any field defect, including mimicking a stroke, a point valuable to ophthalmologists and medics alike.
2015 BMJ Publishing Group Ltd.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous