

Individual Organ Failure and Concomitant Risk of Mortality Differs According to the Type of Admission to ICU - A Retrospective Study of SOFA Score of 23,795 Patients
- PMID: 26241475
- PMCID: PMC4524700
- DOI: 10.1371/journal.pone.0134329
Individual Organ Failure and Concomitant Risk of Mortality Differs According to the Type of Admission to ICU - A Retrospective Study of SOFA Score of 23,795 Patients
Abstract
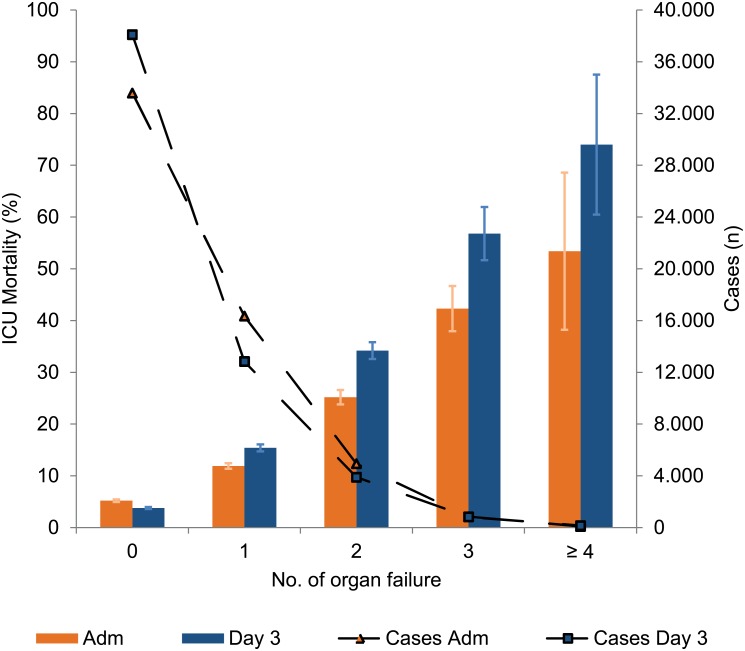
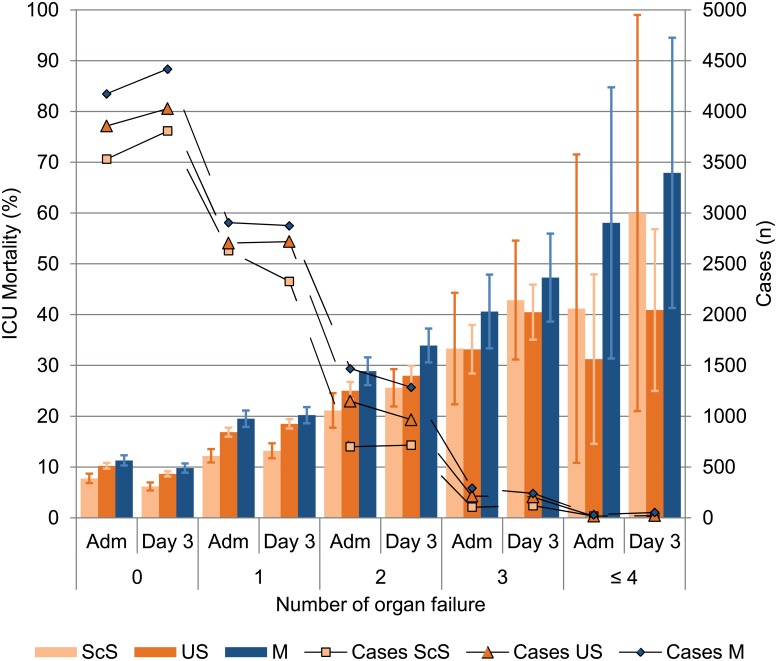
Introduction: Organ dysfunction or failure after the first days of ICU treatment and subsequent mortality with respect to the type of intensive care unit (ICU) admission is poorly elucidated. Therefore we analyzed the association of ICU mortality and admission for medical (M), scheduled surgery (ScS) or unscheduled surgery (US) patients mirrored by the occurrence of organ dysfunction/failure (OD/OF) after the first 72h of ICU stay.
Methods: For this retrospective cohort study (23,795 patients; DIVI registry; German Interdisciplinary Association for Intensive Care Medicine (DIVI)) organ dysfunction or failure were derived from the Sequential Organ Failure Assessment (SOFA) score (excluding the Glasgow Coma Scale). SOFA scores were collected on admission to ICU and 72h later. For patients with a length of stay of at least five days, a multivariate analysis was performed for individual OD/OF on day three.
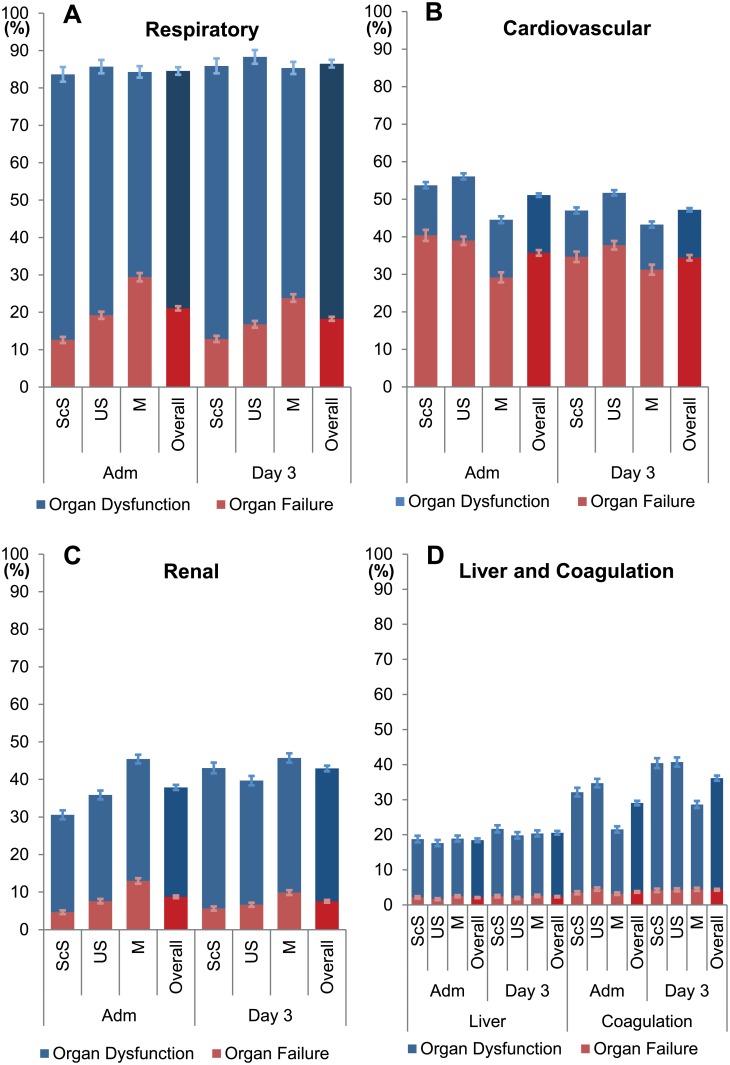
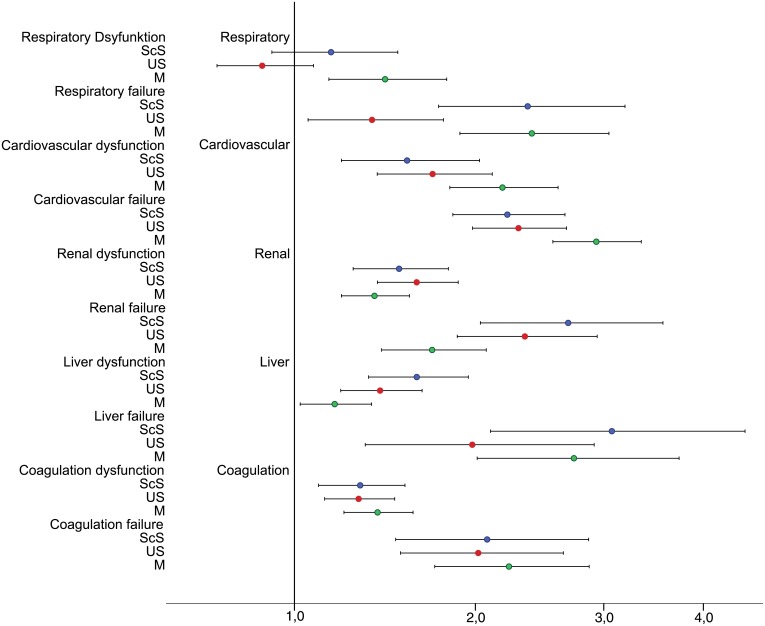
Results: M patients had the lowest prevalence of cardiovascular failure (M 31%; ScS 35%; US 38%), and the highest prevalence of respiratory (M 24%; ScS 13%; US 17%) and renal failure (M 10%; ScS 6%; US 7%). Risk of death was highest for M- and ScS-patients in those with respiratory failure (OR; M 2.4; ScS 2.4; US 1.4) and for surgical patients with renal failure (OR; M 1.7; ScS 2.7; US 2.4).
Conclusion: The dynamic evolution of OD/OF within 72h after ICU admission and mortality differed between patients depending on their types of admission. This has to be considered to exclude a systematic bias during multi-center trials.
Conflict of interest statement
Figures

References
-
- Le Gall JR, Lemeshow S, Saulnier F. A new Simplified Acute Physiology Score (SAPS II) based on a European/North American multicenter study. JAMA: the journal of the American Medical Association. 1993;270(24):2957–63. Epub 1993/12/22. . - PubMed
-
- Moreno RP, Metnitz PG, Almeida E, Jordan B, Bauer P, Campos RA, et al. SAPS 3—From evaluation of the patient to evaluation of the intensive care unit. Part 2: Development of a prognostic model for hospital mortality at ICU admission. Intensive care medicine. 2005;31(10):1345–55. Epub 17 August 2005. 10.1007/s00134-005-2763-5 - DOI - PMC - PubMed
-
- Knaus WA, Wagner DP, Draper EA, Zimmerman JE, Bergner M, Bastos PG, et al. The APACHE III prognostic system. Risk prediction of hospital mortality for critically ill hospitalized adults. Chest. 1991;100(6):1619–36. Epub 1991/12/01. . - PubMed
-
- Vincent JL, Moreno R, Takala J, Willats S. The SOFA (Sepsis. related Organ Failure Assessment) score to describe organ dysfunction/failure. Intensive care medicine. 1996;22:707–10. - PubMed
-
- Vincent JL, de Mendonca A, Cantraine F, Moreno R, Takala J, Suter PM, et al. Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units: results of a multicenter, prospective study. Working group on "sepsis-related problems" of the European Society of Intensive Care Medicine. Critical care medicine. 1998;26(11):1793–800. Epub 1998/11/21. . - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
