

Acute exacerbations of chronic obstructive pulmonary disease are associated with decreased CD4+ & CD8+ T cells and increased growth & differentiation factor-15 (GDF-15) in peripheral blood
- PMID: 26243260
- PMCID: PMC4531816
- DOI: 10.1186/s12931-015-0251-1
Acute exacerbations of chronic obstructive pulmonary disease are associated with decreased CD4+ & CD8+ T cells and increased growth & differentiation factor-15 (GDF-15) in peripheral blood
Abstract
Background: Although T cells, especially CD8+, have been implicated in chronic obstructive pulmonary disease (COPD) pathogenesis, their role during acute exacerbations (AE-COPD) is uncertain.
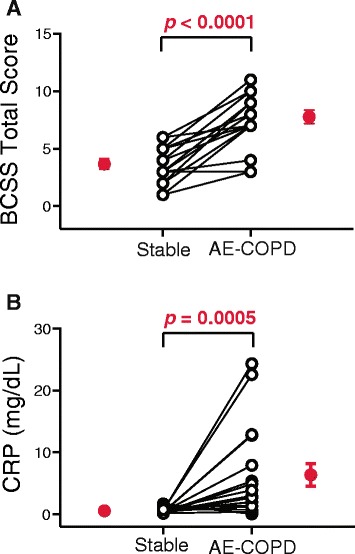
Methods: We recruited subjects with COPD and a history of previous AE-COPD and studied them quarterly to collect blood and spontaneously expectorated sputum while stable. During exacerbations (defined by a change in symptoms plus physician diagnosis and altered medications), we collected blood and sputum before administering antibiotics or steroids. We used flow cytometry to identify leukocytes in peripheral blood, plus Luminex® analysis or ELISA to determine levels of inflammatory biomarkers in serum and sputum supernatants.
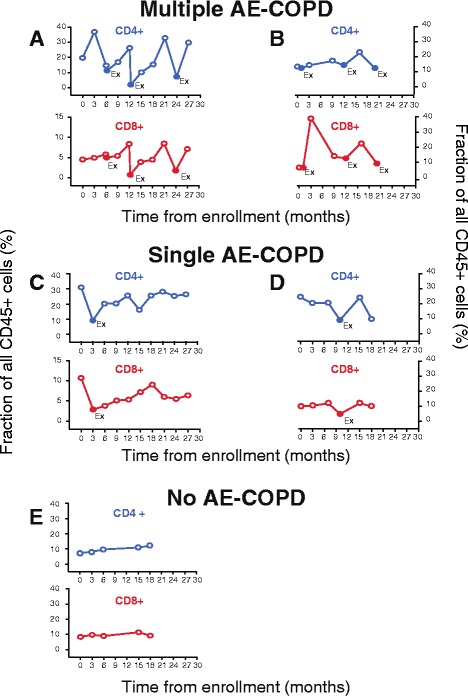
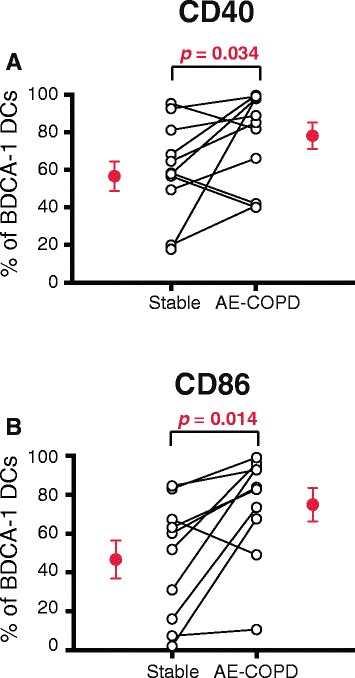
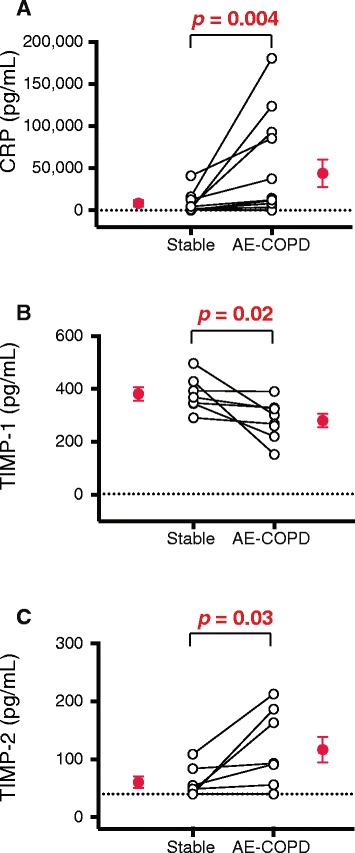
Results: Of 33 enrolled subjects, 13 participated in multiple stable visits and had ≥1 AE-COPD visit, yielding 18 events with paired data. Flow cytometric analyses of peripheral blood demonstrated decreased CD4+ and CD8+ T cells during AE-COPD (both absolute and as a percentage of all leukocytes) and significantly increased granulocytes, all of which correlated significantly with serum C-reactive protein (CRP) concentrations. No change was observed in other leukocyte populations during AE-COPD, although the percentage of BDCA-1+ dendritic cells expressing the activation markers CD40 and CD86 increased. During AE-COPD, sICAM-1, sVCAM-1, IL-10, IL-15 and GDF-15 increased in serum, while in sputum supernatants, CRP and TIMP-2 increased and TIMP-1 decreased.
Conclusions: The decrease in CD4+ and CD8+ T cells (but not other lymphocyte subsets) in peripheral blood during AE-COPD may indicate T cell extravasation into inflammatory sites or organized lymphoid tissues. GDF-15, a sensitive marker of cardiopulmonary stress that in other settings independently predicts reduced long-term survival, is acutely increased in AE-COPD. These results extend the concept that AE-COPD are systemic inflammatory events to which adaptive immune mechanisms contribute.
Trial registration: NCT00281216 , ClinicalTrials.gov.
Figures


References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- UL1 TR000433/TR/NCATS NIH HHS/United States
- T32 HL007749/HL/NHLBI NIH HHS/United States
- P30 CA46952/CA/NCI NIH HHS/United States
- I01 BX001389/BX/BLRD VA/United States
- R01 HL082480/HL/NHLBI NIH HHS/United States
- N01 HR046162/HR/NHLBI NIH HHS/United States
- K24 HL04212/HL/NHLBI NIH HHS/United States
- I01 CX000911/CX/CSRD VA/United States
- K24 HL004212/HL/NHLBI NIH HHS/United States
- T32 HL07749/HL/NHLBI NIH HHS/United States
- U01 HL098961/HL/NHLBI NIH HHS/United States
- N01HR046162/HR/NHLBI NIH HHS/United States
- KL2 RR024987/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
