

"Right place at the right time" impacts outcomes for acute intestinal obstruction
- PMID: 26243347
- PMCID: PMC5169167
- DOI: 10.1016/j.surg.2015.06.032
"Right place at the right time" impacts outcomes for acute intestinal obstruction
Abstract
Background: The purpose of this study was to measure how the duration of nonoperative intervention for intestinal obstruction impacted patient outcomes and whether hospital characteristics influenced the timing of operative intervention.
Methods: The State Inpatient Database (Florida) of the Health Care Utilization Project and the Annual Survey database of the American Hospital Association were linked from 2006 to 2011. Included were patients ≥18 years of age with a primary diagnosis of intestinal obstruction. Patient factors included age, sex, socioeconomic factors, and comorbid conditions.
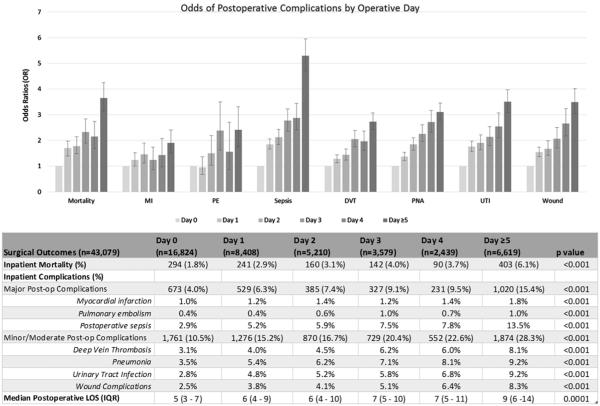
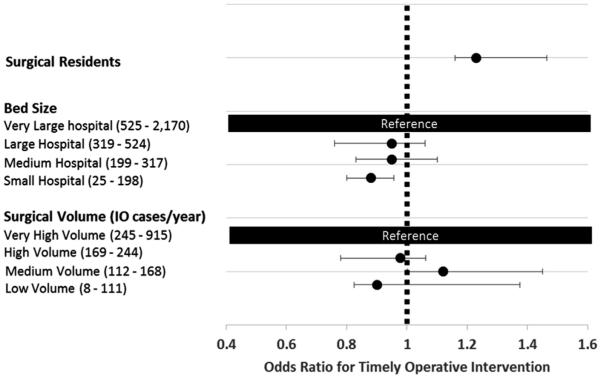
Results: A total of 116,195 patients met our inclusion criteria, and 43,079 underwent operative intervention (37.1%). Patients who required operative correction of the intestinal obstruction after the fifth day of hospitalization, compared with patients who underwent an operation on the day of admission, had increases in mortality (6.1% vs 1.8%, P < .001), complication rates (15.4% vs 4.0%, P < .001), and postoperative hospital stay (9 vs 5 days, P < .001). Patients cared for at a large teaching facility (with surgery residents) had increased odds of early operative intervention by 23% (odds ratio 1.23, [1.20-1.28]), whereas patients at low-volume hospitals had decreased odds of early intervention (odds ratio 0.88, [0.73-0.91]).
Conclusion: Initial nonoperative treatment in patients with uncomplicated intestinal obstruction is an important strategy, but the odds of having an adverse event increase as intestinal obstruction is delayed. Importantly, the presence of surgery residents and increasing bed size are hospital characteristics associated with earlier operative intervention, suggesting a quality benefit for care at large teaching hospitals.
Copyright © 2015 Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Early operation is associated with a survival benefit for patients with adhesive bowel obstruction.Ann Surg. 2013 Sep;258(3):459-65. doi: 10.1097/SLA.0b013e3182a1b100. Ann Surg. 2013. PMID: 24022438
-
Outcomes after emergency general surgery at teaching versus nonteaching hospitals.J Trauma Acute Care Surg. 2015 Jan;78(1):69-76; discussion 76-7. doi: 10.1097/TA.0000000000000493. J Trauma Acute Care Surg. 2015. PMID: 25539205
-
Postoperative outcomes in patients with perforated bowel: early versus late intervention.J Surg Res. 2016 Jun 1;203(1):75-81. doi: 10.1016/j.jss.2016.03.023. Epub 2016 Mar 25. J Surg Res. 2016. PMID: 27338537
-
Operative Treatment of Acute Intestinal Obstruction.Daniels Tex Med J. 1885 Oct;1(4):176-178. Daniels Tex Med J. 1885. PMID: 36953530 Free PMC article. Review. No abstract available.
-
A Review of Acute Intestinal Obstruction.Med J Southwest. 1959 Apr;74(2):31-39. Med J Southwest. 1959. PMID: 28907916 Free PMC article. Review. No abstract available.
Cited by
-
Outcomes After Surgery for Benign and Malignant Small Bowel Obstruction.J Gastrointest Surg. 2017 Feb;21(2):363-371. doi: 10.1007/s11605-016-3307-8. Epub 2016 Oct 25. J Gastrointest Surg. 2017. PMID: 27783343 Free PMC article.
-
Adhesive Bowel Obstruction Following Urologic Surgery: Improved Outcomes with Early Intervention.Curr Urol. 2018 Jun;11(4):175-181. doi: 10.1159/000447215. Epub 2018 Mar 30. Curr Urol. 2018. PMID: 29997459 Free PMC article.
-
Longer Trials of Non-operative Management for Adhesive Small Bowel Obstruction Are Associated with Increased Complications.J Gastrointest Surg. 2020 Apr;24(4):890-898. doi: 10.1007/s11605-019-04156-6. Epub 2019 May 6. J Gastrointest Surg. 2020. PMID: 31062274
-
Long-term hospital mortality due to small bowel obstruction after major colorectal surgery in a national cohort database.Int J Colorectal Dis. 2019 Feb;34(2):329-336. doi: 10.1007/s00384-018-3200-x. Epub 2018 Nov 26. Int J Colorectal Dis. 2019. PMID: 30478639
-
Comparisons of the surgical outcomes and medical costs between transferred and directly admitted patients diagnosed with intestinal obstruction in an American tertiary referral center.Int J Colorectal Dis. 2018 Nov;33(11):1617-1625. doi: 10.1007/s00384-018-3052-4. Epub 2018 Apr 20. Int J Colorectal Dis. 2018. PMID: 29679151
References
-
- Miller G, Boman J, Shrier I, Gordon PH. Etiology of small bowel obstruction. Am J Surg. 2000;180:33–6. - PubMed
-
- Hayanga AJ, Bass-Wilkins K, Bulkley GB. Current management of small-bowel obstruction. Adv Surg. 2005;39:1–33. - PubMed
-
- Teixeira PG, Karamanos E, Talving P, Inaba K, Lam L, Demetriades D. Early operation is associated with a survival benefit for patients with adhesive bowel obstruction. Ann Surg. 2013;258:459–65. - PubMed
-
- Malangoni MA, Times ML, Kozik D, Merlino JI. Admitting service influences the outcomes of patients with small bowel obstruction. Surgery. 2001;130:706–13. - PubMed
-
- Bizer LS, Liebling RW, Delany HM, Gliedman ML. Small bowel obstruction: the role of non-operative treatment in simple intestinal obstruction and predictive criteria for strangulation obstruction. Surgery. 1981;89:407–13. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
