

Frailty in Advanced Heart Failure: A Consequence of Aging or a Separate Entity?
- PMID: 26244037
- PMCID: PMC4501712
- DOI: 10.4137/CMC.S19698
Frailty in Advanced Heart Failure: A Consequence of Aging or a Separate Entity?
Abstract
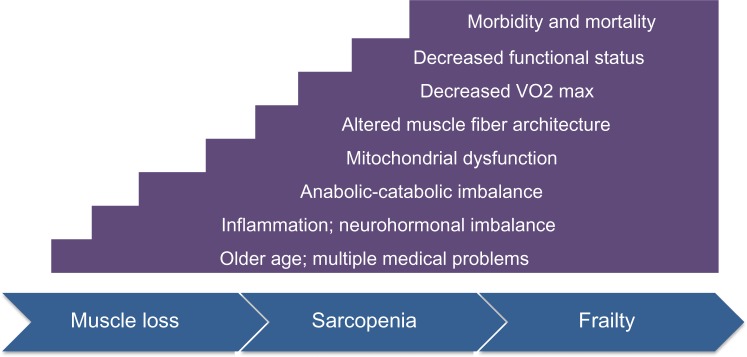
There are over 5 million Americans with heart failure (HF), the majority of whom are over age 65. Frailty is a systemic syndrome associated with aging that produces subclinical dysfunction across multiple organ systems and leads to an increased risk for morbidity and mortality. The prevalence of frailty is about 10% in community-dwelling elderly and 20% in those with advanced HF, and increases in both cohorts with age. Yet the relationship between the primary frailty of aging and frailty secondary to HF remains poorly defined. Whether the frailty of these two populations share similar etiologies or exist as separate entities is unknown. Teasing apart potential molecular, cellular, and functional differences between the frailty of aging and that of advanced HF has implications for risk stratification, quality of life, and pharmacological and therapeutic interventions for advanced HF patients.
Keywords: frailty; geriatric cardiology; heart failure; sarcopenia.
Figures
References
-
- Collard RM, Boter H, Schoevers RA, Oude Voshaar RC. Prevalence of frailty in community-dwelling older persons: a systematic review. J Am Geriatr Soc. 2012;60(8):1487–92. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
