

From variome to phenome: Pathogenesis, diagnosis and management of ectopic mineralization disorders
- PMID: 26244149
- PMCID: PMC4517332
- DOI: 10.12998/wjcc.v3.i7.556
From variome to phenome: Pathogenesis, diagnosis and management of ectopic mineralization disorders
Abstract
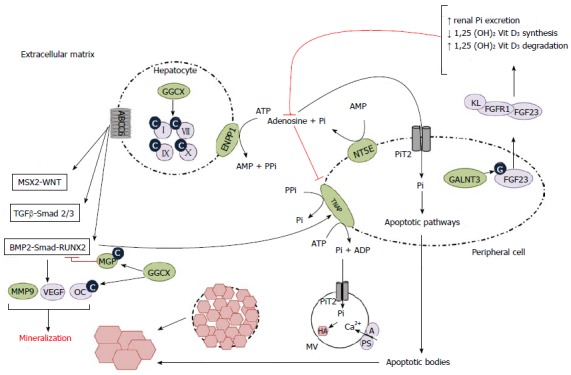
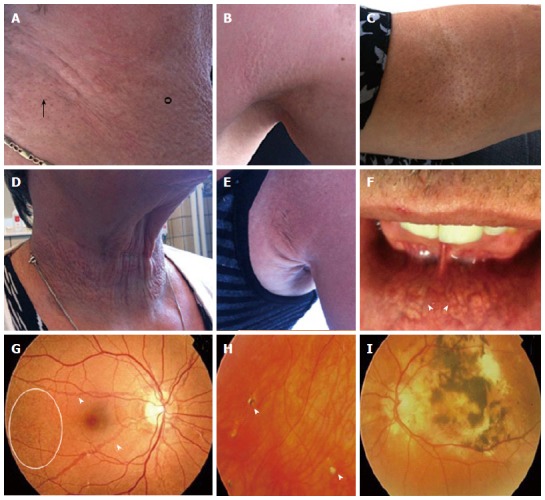
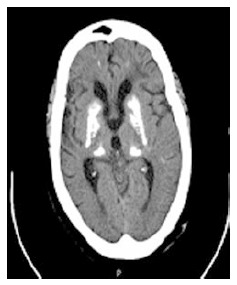
Ectopic mineralization - inappropriate biomineralization in soft tissues - is a frequent finding in physiological aging processes and several common disorders, which can be associated with significant morbidity and mortality. Further, pathologic mineralization is seen in several rare genetic disorders, which often present life-threatening phenotypes. These disorders are classified based on the mechanisms through which the mineralization occurs: metastatic or dystrophic calcification or ectopic ossification. Underlying mechanisms have been extensively studied, which resulted in several hypotheses regarding the etiology of mineralization in the extracellular matrix of soft tissue. These hypotheses include intracellular and extracellular mechanisms, such as the formation of matrix vesicles, aberrant osteogenic and chondrogenic signaling, apoptosis and oxidative stress. Though coherence between the different findings is not always clear, current insights have led to improvement of the diagnosis and management of ectopic mineralization patients, thus translating pathogenetic knowledge (variome) to the phenotype (phenome). In this review, we will focus on the clinical presentation, pathogenesis and management of primary genetic soft tissue mineralization disorders. As examples of dystrophic calcification disorders Pseudoxanthoma elasticum, Generalized arterial calcification of infancy, Keutel syndrome, Idiopathic basal ganglia calcification and Arterial calcification due to CD73 (NT5E) deficiency will be discussed. Hyperphosphatemic familial tumoral calcinosis will be reviewed as an example of mineralization disorders caused by metastatic calcification.
Keywords: Arterial calcification due to CD73 deficiency; Ectopic mineralization; Etiology; Generalized arterial calcification of infancy; Hyperphosphatemic familial tumoral calcinosis; Idiopathic basal ganglia calcification; Keutel syndrome; Phenotype; Pseudoxanthoma elasticum; Pseudoxanthoma elasticum-like syndrome.
Figures

References
-
- Vanakker O, Hosen MJ, De Paepe A. Ectopic soft tissue calcification: process, determinants and health impact. Hauppauge, NY: Human Anatomy and Physiology; 2013. pp. 261–304.
-
- Kirsch T. Biomineralization--an active or passive process? Connect Tissue Res. 2012;53:438–445. - PubMed
-
- Kornak U. Animal models with pathological mineralization phenotypes. Joint Bone Spine. 2011;78:561–567. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
