

Efficacy and Safety of Alfuzosin as Medical Expulsive Therapy for Ureteral Stones: A Systematic Review and Meta-Analysis
- PMID: 26244843
- PMCID: PMC4526635
- DOI: 10.1371/journal.pone.0134589
Efficacy and Safety of Alfuzosin as Medical Expulsive Therapy for Ureteral Stones: A Systematic Review and Meta-Analysis
Abstract
Background: Alfuzosin has been widely used to treat benign prostatic hyperplasia and prostatitis, and is claimed to be a selective agent for the lower urinary tract with low incidence of adverse side-effects and hypotensive changes. Recently, several randomized controlled trials have reported using Alfuzosin as an expulsive therapy of ureteral stones. Tamsulosin, another alpha blocker, has also been used as an agent for the expulsive therapy for ureteral stones. It is unclear whether alfuzosin has similar efficacy as Tamsulosin in the management of ureteral stones.
Objective: To perform a systematic review and analysis of literatures comparing Alfuzosin with Tamsulosin or standard conservative therapy for the treatment of ureteral stones less than 10 mm in diameter.
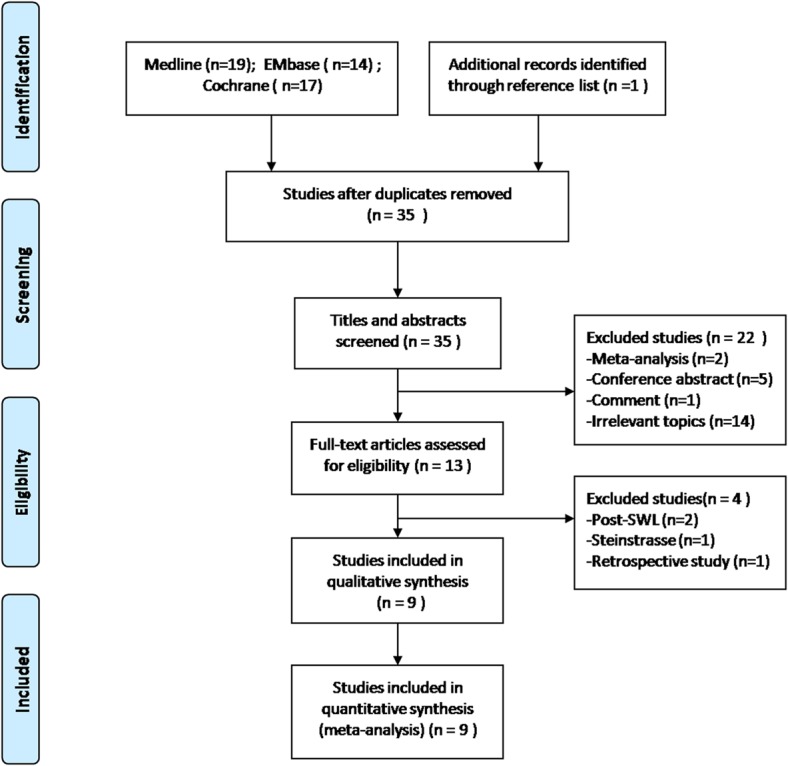
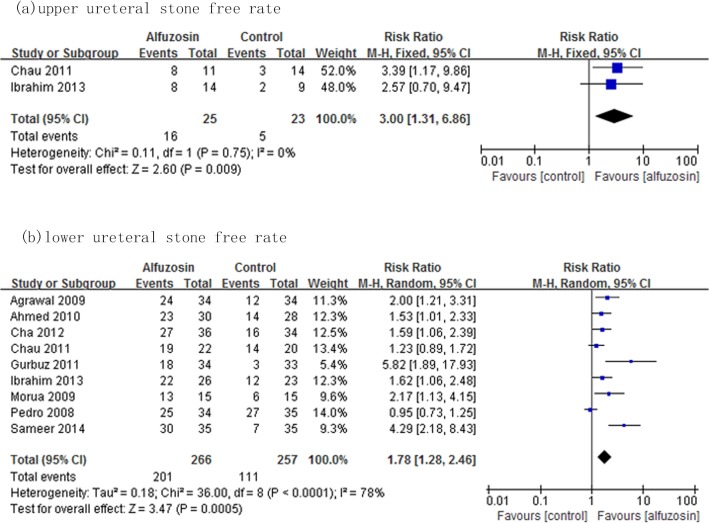
Methods: A systematic literature review was performed in December 2014 using Pubmed, Embase, and the Cochrane library databases to identify relevant studies. All randomized and controlled trials were included. A subgroup analysis was performed comparing Alfuzosin with control therapy on the management of distal ureteral stones.
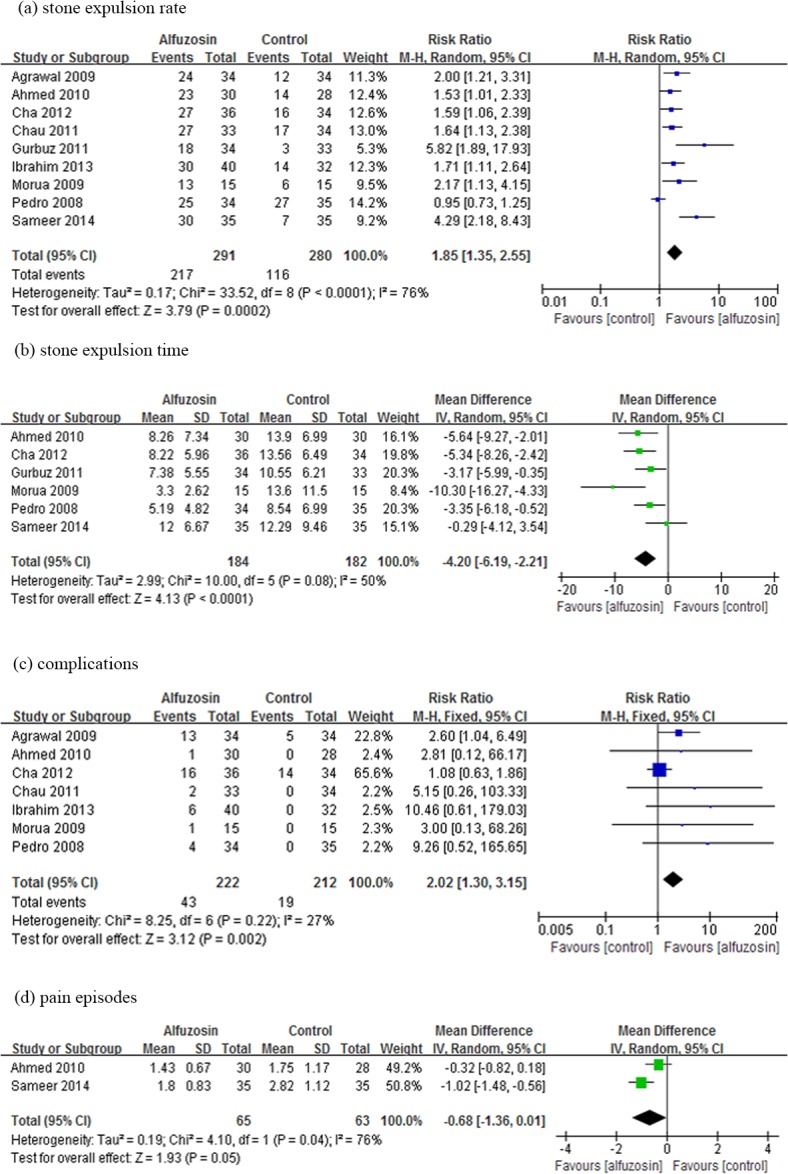
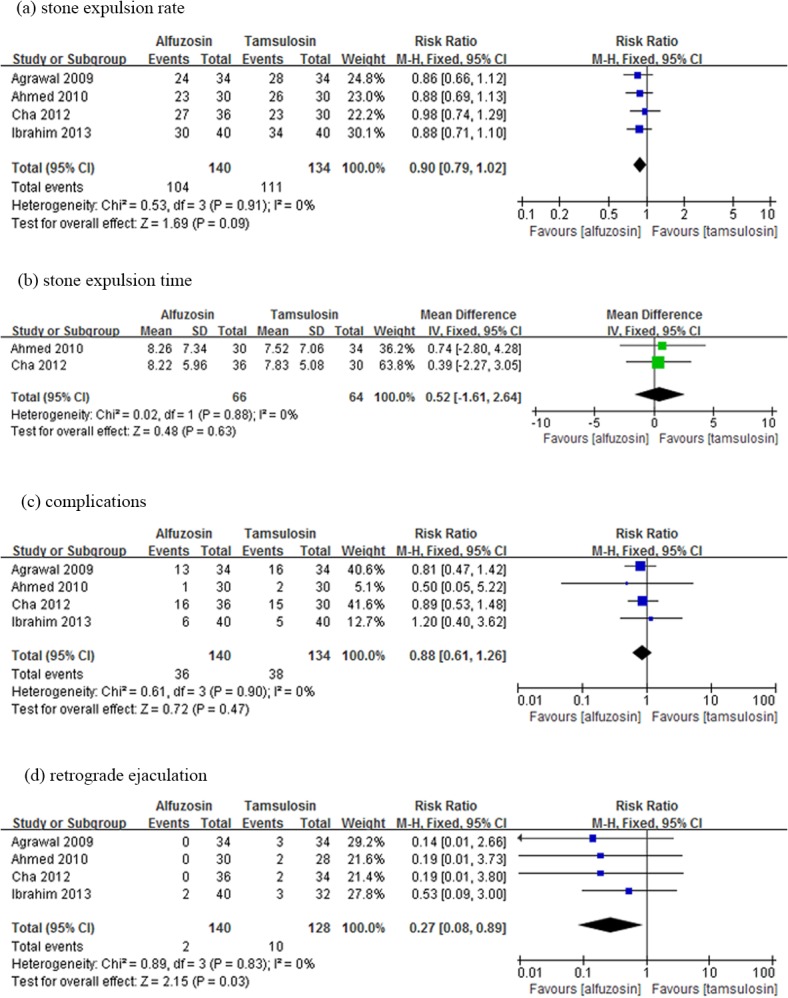
Results: Alfuzosin provided a significantly higher stone-free rate than the control treatments (RR: 1.85; 95% confidence interval [CI], 1.35-2.55; p<0.001), and a shorter stone expulsion time (Weighted mean difference [WMD]: -4.20 d, 95%CI, -6.19 to -2.21; p<0.001), but it has a higher complication rate (RR: 2.02; 95% CI, 1.30-3.15; p<0.01). When Alfuzosin was compared to Tamsulosin, there was no significant difference in terms of stone-free rate (RR: 0.90; 95% CI, 0.79-1.02; p = 0.09) as well as the stone expulsion time (WMD: 0.52 d, 95%CI, -1.61 to 2.64; p = 0.63). The adverse effects of Alfuzosin were similar to those of Tamsulosin (RR: 0.88; 95% CI, 0.61-1.26; p = 0.47).
Conclusions: Alfuzosin is a safe and effective agent for the expulsive therapy of ureteral stones smaller than 10 mm in size. It is more effective than therapeutic regiment without alpha blocker. It is equivalent to Tamsulosin in its effectiveness and safety profile. Adverse effects should always be kept in mind when use this class of drugs.
Conflict of interest statement
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
