

Telephone-Delivered Cognitive Behavioral Therapy and Telephone-Delivered Nondirective Supportive Therapy for Rural Older Adults With Generalized Anxiety Disorder: A Randomized Clinical Trial
- PMID: 26244854
- PMCID: PMC4939613
- DOI: 10.1001/jamapsychiatry.2015.1154
Telephone-Delivered Cognitive Behavioral Therapy and Telephone-Delivered Nondirective Supportive Therapy for Rural Older Adults With Generalized Anxiety Disorder: A Randomized Clinical Trial
Abstract
Importance: Generalized anxiety disorder (GAD) is common in older adults; however, access to treatment may be limited, particularly in rural areas.
Objective: To examine the effects of telephone-delivered cognitive behavioral therapy (CBT) compared with telephone-delivered nondirective supportive therapy (NST) in rural older adults with GAD.
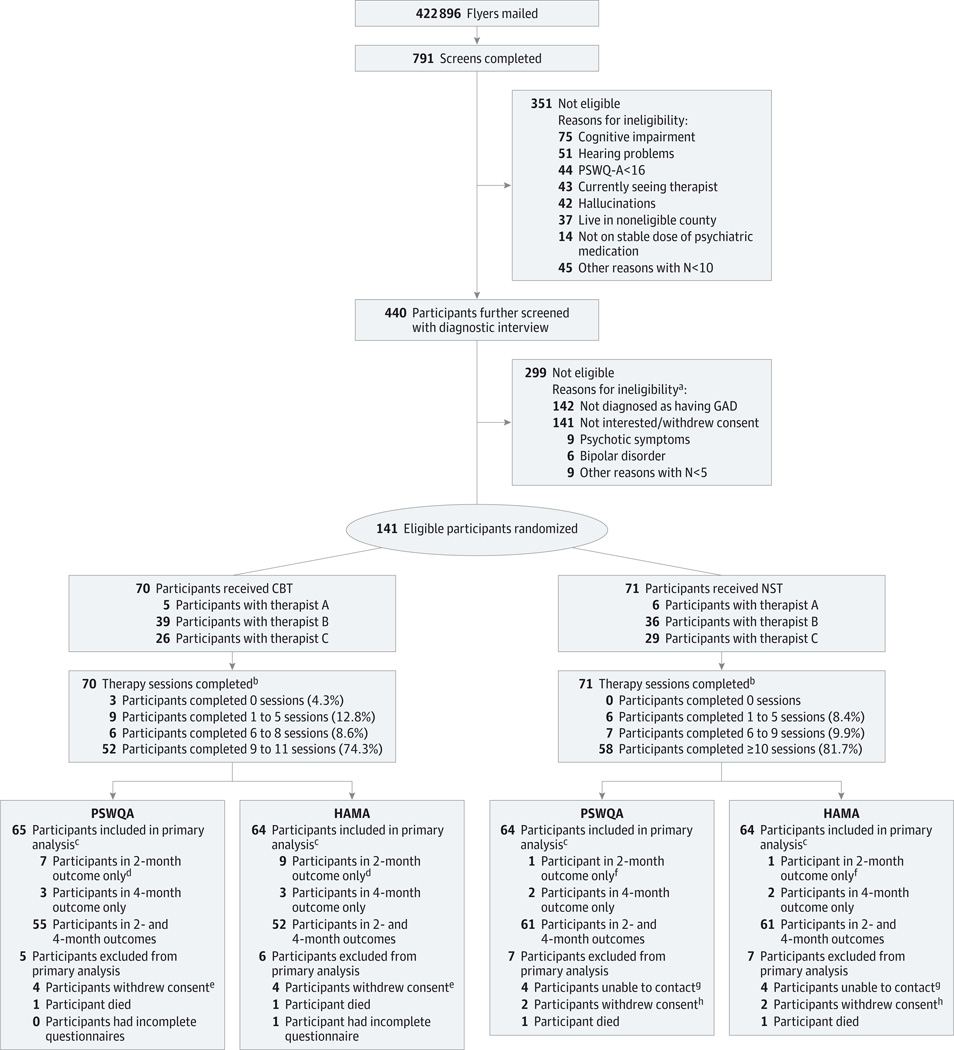
Design, setting, and participants: Randomized clinical trial in the participants' homes of 141 adults aged 60 years and older with a principal or coprincipal diagnosis of GAD who were recruited between January 27, 2011, and October 22, 2013.
Interventions: Telephone-delivered CBT consisted of as many as 11 sessions (9 were required) focused on recognition of anxiety symptoms, relaxation, cognitive restructuring, the use of coping statements, problem solving, worry control, behavioral activation, exposure therapy, and relapse prevention, with optional chapters on sleep and pain. Telephone-delivered NST consisted of 10 sessions focused on providing a supportive atmosphere in which participants could share and discuss their feelings and did not provide any direct suggestions for coping.
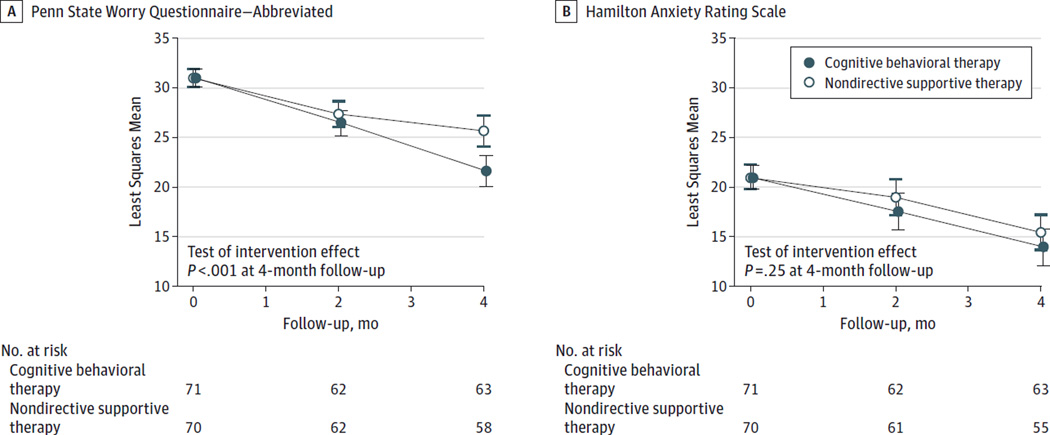
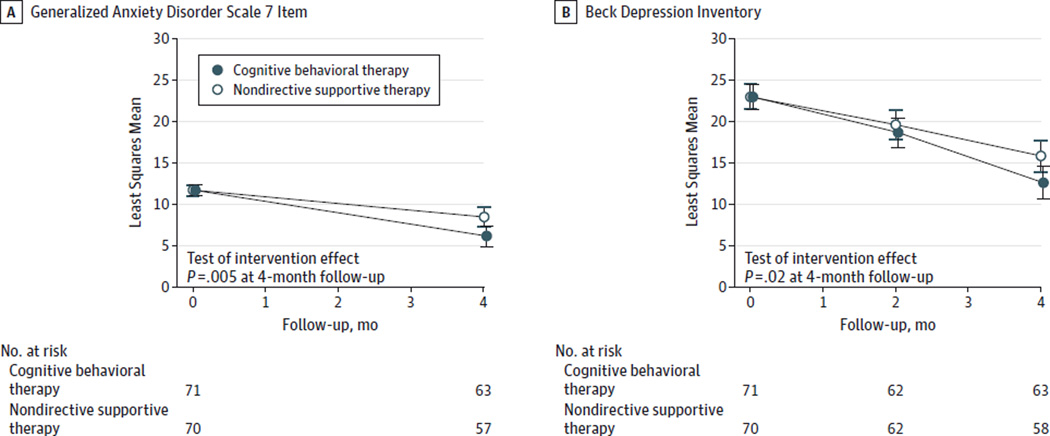
Main outcomes and measures: Primary outcomes included interviewer-rated anxiety severity (Hamilton Anxiety Rating Scale) and self-reported worry severity (Penn State Worry Questionnaire-Abbreviated) measured at baseline, 2 months' follow-up, and 4 months' follow-up. Mood-specific secondary outcomes included self-reported GAD symptoms (GAD Scale 7 Item) measured at baseline and 4 months' follow-up and depressive symptoms (Beck Depression Inventory) measured at baseline, 2 months' follow-up, and 4 months' follow-up. Among the 141 participants, 70 were randomized to receive CBT and 71 to receive NST.
Results: At 4 months' follow-up, there was a significantly greater decline in worry severity among participants in the telephone-delivered CBT group (difference in improvement, -4.07; 95% CI, -6.26 to -1.87; P = .004) but no significant differences in general anxiety symptoms (difference in improvement, -1.52; 95% CI, -4.07 to 1.03; P = .24). At 4 months' follow-up, there was a significantly greater decline in GAD symptoms (difference in improvement, -2.36; 95% CI, -4.00 to -0.72; P = .005) and depressive symptoms (difference in improvement, -3.23; 95% CI, -5.97 to -0.50; P = .02) among participants in the telephone-delivered CBT group.
Conclusions and relevance: In this trial, telephone-delivered CBT was superior to telephone-delivered NST in reducing worry, GAD symptoms, and depressive symptoms in older adults with GAD.
Trial registration: clinicaltrials.gov Identifier: NCT01259596.
Conflict of interest statement
Figures
Comment in
-
Solving the Geriatric Mental Health Crisis in the 21st Century.JAMA Psychiatry. 2015 Oct;72(10):967-8. doi: 10.1001/jamapsychiatry.2015.1306. JAMA Psychiatry. 2015. PMID: 26244750 No abstract available.
-
Letter to Editor. Is it possible to support cognitive behavioral therapy, led remotely, by determining so-called therapeutic tasks?Psychiatr Pol. 2015;49(6):1373-7. doi: 10.12740/PP/59543. Psychiatr Pol. 2015. PMID: 26909409 English, Polish.
References
-
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th. Washington, DC: American Psychiatric Association; 2000.
-
- Mantella RC, Butters MA, Dew MA, et al. Cognitive impairment in late-life generalized anxiety disorder. Am J Geriatr Psychiatry. 2007;15(8):673–679. - PubMed
-
- Carrière I, Ryan J, Norton J, et al. Anxiety and mortality risk in community-dwelling elderly people. Br J Psychiatry. 2013;203(3):303–309. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
